

ERas and COLorectal endoscopic surgery: an Italian society for endoscopic surgery and new technologies (SICE) national report
- PMID: 35501602
- PMCID: PMC9485180
- DOI: 10.1007/s00464-022-09212-y
ERas and COLorectal endoscopic surgery: an Italian society for endoscopic surgery and new technologies (SICE) national report
Erratum in
-
Correction: ERas and COLorectal endoscopic surgery: an Italian society for endoscopic surgery and new technologies (SICE) national report.Surg Endosc. 2022 Oct;36(10):7628. doi: 10.1007/s00464-022-09344-1. Surg Endosc. 2022. PMID: 35608700 Free PMC article. No abstract available.
Abstract
Background: Several reports demonstrated a strong association between the level of adherence to the protocol and improved clinical outcomes after surgery. However, it is difficult to obtain full adherence to the protocol into clinical practice and has still not been identified the threshold beyond which improved functional results can be reached.
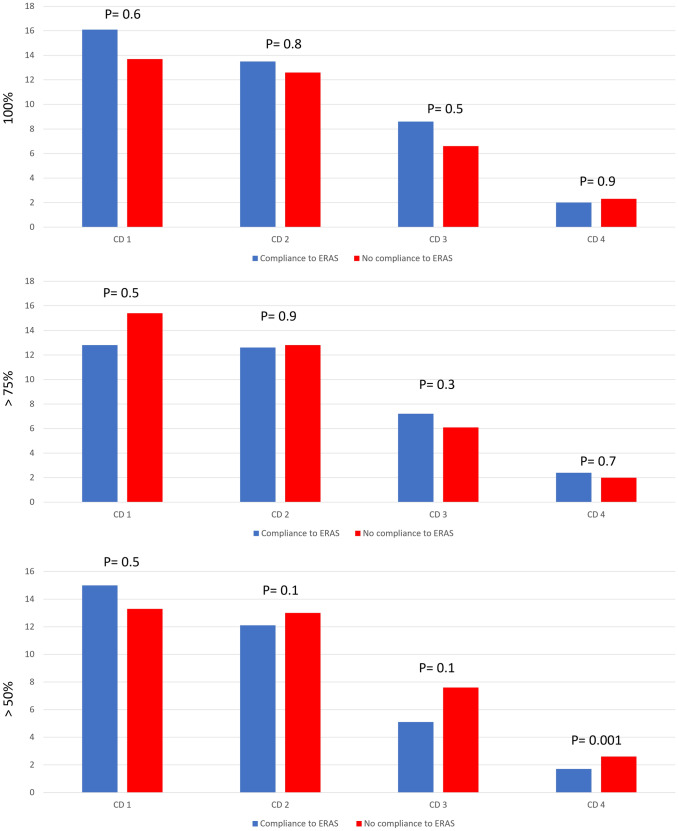
Methods: The ERCOLE (ERas and COLorectal Endoscopic surgery) study was as a cohort, prospective, multi-centre national study evaluating the association between adherence to ERAS items and clinical outcomes after minimally invasive colorectal surgery. The primary endpoint was to associate the percentage of ERAS adherence to functional recovery after minimally invasive colorectal cancer surgery. The secondary endpoints of the study was to validate safety of the ERAS programme evaluating complications' occurrence according to Clavien-Dindo classification and to evaluate the compliance of the Italian surgeons to each ERAS item.
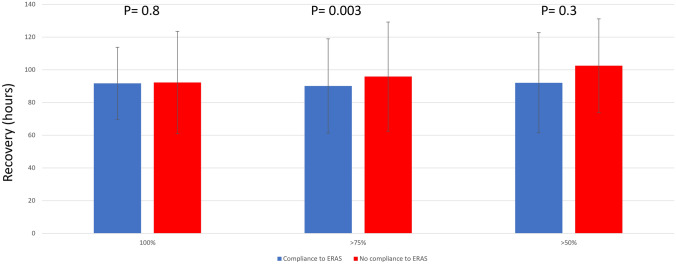
Results: 1138 patients were included. Adherence to the ERAS protocol was full only in 101 patients (8.9%), > 75% of the ERAS items in 736 (64.7%) and > 50% in 1127 (99%). Adherence to > 75% was associated with a better functional recovery with 90.2 ± 98.8 vs 95.9 ± 33.4 h (p = 0.003). At difference, full adherence to the ERAS components 91.7 ± 22.1 vs 92.2 ± 31.6 h (p = 0.8) was not associated with better recovery.
Conclusions: Our results were encouraging to affirm that adherence to the ERAS program up to 75% could be considered satisfactory to get the goal. Our study could be considered a call to simplify the ERAS protocol facilitating its penetrance into clinical practice.
Keywords: Colorectal; ERAS; Enhanced Recovery; Minimally invasive.
© 2022. The Author(s).
Conflict of interest statement
Marco Milone, Ugo Elmore, Michele Manigrasso, Monica Ortenzi, Emanuele Botteri, Alberto Arezzo, Gianfranco Silecchia, Mario Guerrieri, Giovanni Domenico De Palma and Ferdinando Agresta have no conflicts of interest or financial ties to disclose.
Figures
References
-
- Nygren J, Thacker J, Carli F, Fearon KCH, Norderval S, Lobo DN, Ljungqvist O, Soop M, Ramirez J. Guidelines for perioperative care in elective rectal/pelvic surgery: enhanced recovery after surgery (ERAS®) society recommendations. World J Surg. 2013;37:285–305. doi: 10.1007/s00268-012-1787-6. - DOI - PubMed
-
- Gustafsson UO, Scott MJ, Schwenk W, Demartines N, Roulin D, Francis N, McNaught CE, MacFie J, Liberman AS, Soop M, Hill A, Kennedy RH, Lobo DN, Fearon K, Ljungqvist O. Guidelines for perioperative care in elective colonic surgery: enhanced recovery after surgery (ERAS®) society recommendations. World J Surg. 2013;37:259–284. doi: 10.1007/s00268-012-1772-0. - DOI - PubMed
-
- Vignali A, Elmore U, Guarneri G, De Ruvo V, Parise P, Rosati R. Enhanced recovery after surgery in colon and rectal surgery: identification of predictive variables of failure in a monocentric series including 733 patients. Updates Surg. 2021;73(1):111–121. doi: 10.1007/s13304-020-00848-w. - DOI - PubMed
-
- Maessen J, Dejong CHC, Hausel J, Nygren J, Lassen K, Andersen J, Kessels AGH, Revhaug A, Kehlet H, Ljungqvist O, Fearon KCH, Von Meyenfeldt MF. A protocol is not enough to implement an enhanced recovery programme for colorectal resection. Br J Surg. 2007;94:224–231. doi: 10.1002/bjs.5468. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
