

Robotic-assisted minimally invasive Ivor Lewis esophagectomy within the prospective multicenter German da Vinci Xi registry trial
- PMID: 35501604
- PMCID: PMC9283356
- DOI: 10.1007/s00423-022-02520-w
Robotic-assisted minimally invasive Ivor Lewis esophagectomy within the prospective multicenter German da Vinci Xi registry trial
Abstract
Purpose: Robotic-assisted minimally invasive esophagectomy (RAMIE) has become one standard approach for the operative treatment of esophageal tumors at specialized centers. Here, we report the results of a prospective multicenter registry for standardized RAMIE.
Methods: The German da Vinci Xi registry trial included all consecutive patients who underwent RAMIE at five tertiary university centers between Oct 17, 2017, and Jun 5, 2020. RAMIE was performed according to a standard technique using an intrathoracic circular stapled esophagogastrostomy.
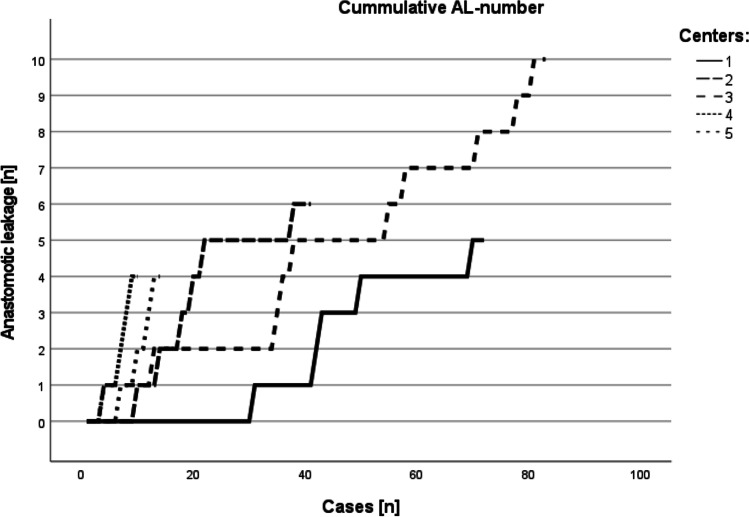
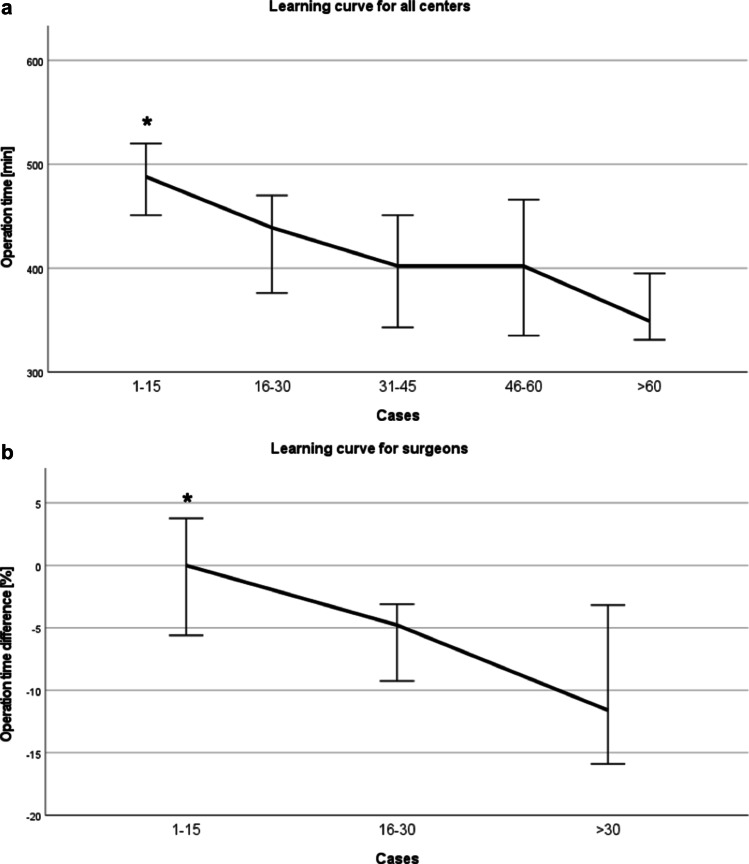
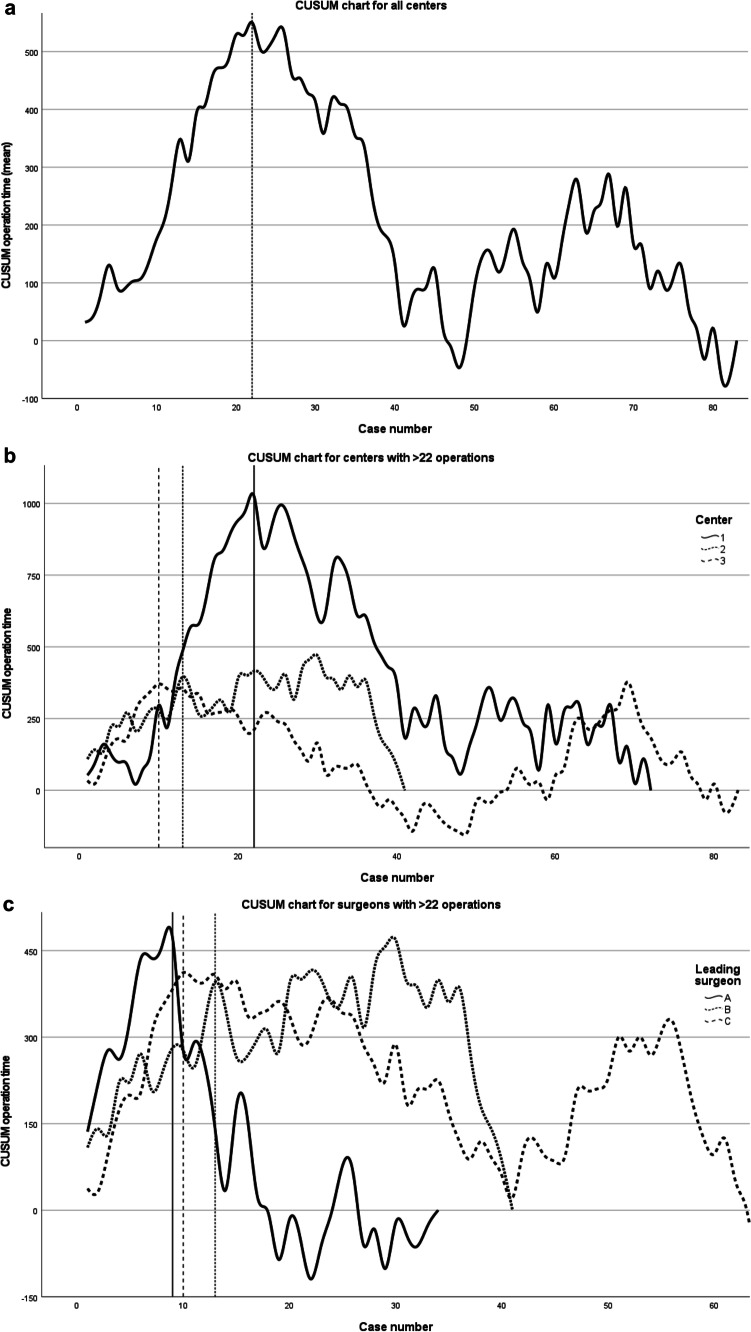
Results: A total of 220 patients were included. The median age was 64 years. Total minimally invasive RAMIE was accomplished in 85.9%; hybrid resection with robotic-assisted thoracic approach was accomplished in an additional 11.4%. A circular stapler size of ≥28 mm was used in 84%, and the median blood loss and operative time were 200 (IQR: 80-400) ml and 425 (IQR: 335-527) min, respectively. The rate of anastomotic leakage was 13.2% (n=29), whereas the two centers with >70 cases each had rates of 7.0% and 12.0%. Pneumonia occurred in 19.5% of patients, and the 90-day mortality was 3.6%. Cumulative sum analysis of the operative time indicated the end of the learning curve after 22 cases.
Conclusions: High-quality multicenter registry data confirm that RAMIE is a safe procedure and can be reproduced with acceptable leak rates in a multicenter setting. The learning curve is comparably low for experienced robotic surgeons.
Keywords: CUSUM analysis; Esophagectomy; Ivor Lewis; Leaning curve; Multicenter; RAMIE.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Berlth F, Mann C, Uzun E et al (2020) Technical details of the abdominal part during full robotic-assisted minimally invasive esophagectomy. Dis Esophagus 33. 10.1093/dote/doaa084 - PubMed
-
- De Groot EM, Moller T, Kingma BF et al (2020) Technical details of the hand-sewn and circular-stapled anastomosis in robot-assisted minimally invasive esophagectomy. Dis Esophagus 33. 10.1093/dote/doaa055 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
