

Paraneoplastic cerebellar degeneration with anti-Yo antibodies and an associated submandibular gland tumor: a case report
- PMID: 35501715
- PMCID: PMC9059384
- DOI: 10.1186/s12883-022-02684-4
Paraneoplastic cerebellar degeneration with anti-Yo antibodies and an associated submandibular gland tumor: a case report
Abstract
Background: As a debilitating syndrome, paraneoplastic cerebellar degeneration (PCD) remains challenging to treat. Further, anti-Yo antibody (directed against human cerebellar degeneration-related protein 2) detection in patients with PCD is associated with unsatisfactory responses to existing therapies. Here, we present the case of a 60-year-old woman who developed PCD with anti-Yo antibodies and a submandibular gland tumor.
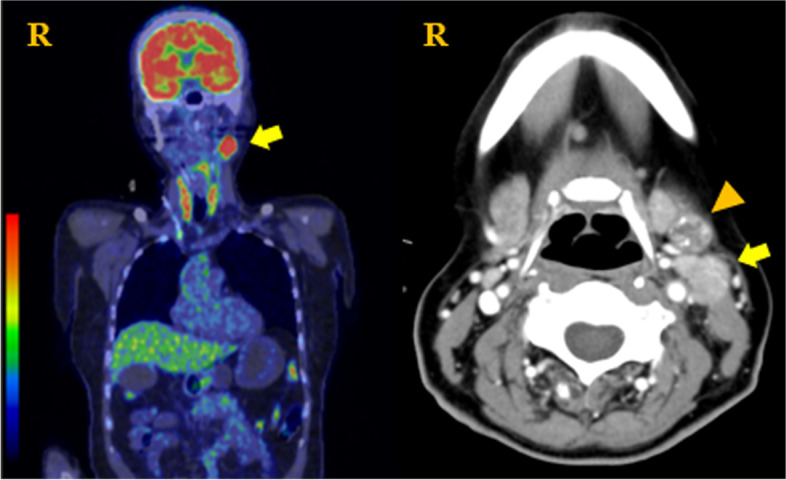
Case presentation: A 60-year-old woman presented with a 5-day history of unsteadiness of gait and inadequate coordination of her extremities, along with truncal instability. Although walking without aid was possible, dysmetria of all four limbs, trunk, and gait ataxia was observed. While routine biochemical and hematological examinations were normal, the patient's blood was positive for anti-Yo antibodies. When the neurological symptoms deteriorated despite administration of intravenous methylprednisolone, fluorodeoxyglucose-positron emission tomography (FDG-PET) and computed tomography (CT) images with contrast enhancement were performed, which showed a tumor in the left submaxillary gland. She underwent total left submandibular gland resection, including the tumor; histological and immunohistochemical results revealed a salivary duct carcinoma. She was administered intravenous methylprednisolone, followed by 10 plasma exchange sessions, intravenous immunoglobulins, and cyclophosphamide therapy. Following treatment, her symptoms were not alleviated, even after the reduction of anti-Yo titers.
Conclusions: Although tumor detection was delayed, early tumor detection, diagnosis, and PCD treatment are essential because any delay can result in the progression of the disorder and irreversible neurological damage. Therefore, we recommend that the possibility of a salivary gland tumor should be considered, and whole-body dual-modality CT, including the head and neck, and FDG-PET should be performed at the earliest for patients with well-characterized paraneoplastic antibodies when conventional imaging fails to identify a tumor.
Keywords: Anti-Yo antibodies; Paraneoplastic cerebellar degeneration; Paraneoplastic syndrome; Salivary duct carcinoma; Submandibular gland tumor.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Case report: paraneoplastic cerebellar degeneration associated with anti-Yo antibody successfully treated with ofatumumab.Front Immunol. 2024 Dec 16;15:1476397. doi: 10.3389/fimmu.2024.1476397. eCollection 2024. Front Immunol. 2024. PMID: 39737186 Free PMC article.
-
A cerebellar degeneration-related protein 2-like cell-based assay for anti-Yo detection in patients with paraneoplastic cerebellar degeneration.Eur J Neurol. 2023 Jun;30(6):1727-1733. doi: 10.1111/ene.15786. Epub 2023 Mar 26. Eur J Neurol. 2023. PMID: 36912432
-
Paraneoplastic cerebellar degeneration associated with antineuronal antibodies: analysis of 50 patients.Brain. 2003 Jun;126(Pt 6):1409-18. doi: 10.1093/brain/awg133. Brain. 2003. PMID: 12764061
-
Plasma exchange for treating anti-Yo-associated paraneoplastic cerebellar degeneration: Case report and literature review.Medicine (Baltimore). 2020 Aug 14;99(33):e21760. doi: 10.1097/MD.0000000000021760. Medicine (Baltimore). 2020. PMID: 32872070 Free PMC article. Review.
-
Anti-Yo antibody-mediated paraneoplastic cerebellar degeneration associated with cognitive affective syndrome in a patient with breast cancer: a case report and literature review.Curr Oncol. 2018 Dec;25(6):e585-e591. doi: 10.3747/co.25.4106. Epub 2018 Dec 1. Curr Oncol. 2018. PMID: 30607127 Free PMC article. Review.
Cited by
-
Posterior reversible encephalopathy syndrome (PRES) in classic Hodgkin's lymphoma, complicated by anthracycline-induced cardiomyopathy.BMJ Case Rep. 2024 Aug 14;17(8):e257523. doi: 10.1136/bcr-2023-257523. BMJ Case Rep. 2024. PMID: 39142839 Free PMC article.
-
Case Report: Anti-Yo antibody mediated paraneoplastic cerebellar degeneration in a patient with squamous cell lung carcinoma.Front Immunol. 2025 Mar 21;16:1558867. doi: 10.3389/fimmu.2025.1558867. eCollection 2025. Front Immunol. 2025. PMID: 40191215 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
