

How to implement geriatric co-management in your hospital? Insights from the G-COACH feasibility study
- PMID: 35501840
- PMCID: PMC9059346
- DOI: 10.1186/s12877-022-03051-1
How to implement geriatric co-management in your hospital? Insights from the G-COACH feasibility study
Abstract
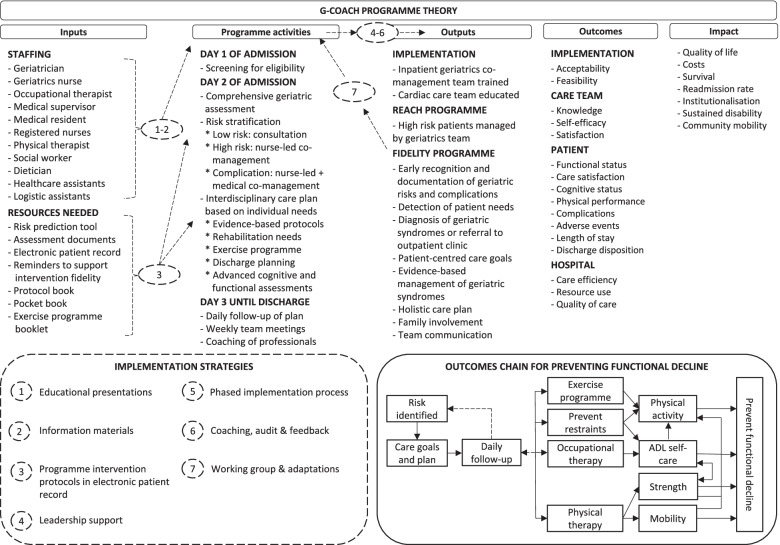
Background: Geriatric co-management is advocated to manage frail patients in the hospital, but there is no guidance on how to implement such programmes in practice. This paper reports our experiences with implementing the 'Geriatric CO-mAnagement for Cardiology patients in the Hospital' (G-COACH) programme. We investigated if G-COACH was feasible to perform after the initial adoption, investigated how well the implementation strategy was able to achieve the implementation targets, determined how patients experienced receiving G-COACH, and determined how healthcare professionals experienced the implementation of G-COACH.
Methods: A feasibility study of the G-COACH programme was performed using a one-group experimental study design. G-COACH was previously implemented on two cardiac care units. Patients and healthcare professionals participating in the G-COACH programme were recruited for this evaluation. The feasibility of the programme was investigated by observing the reach, fidelity and dose using registrations in the electronic patient record and by interviewing patients. The success of the implementation reaching its targets was evaluated using a survey that was completed by 48 healthcare professionals. The experiences of 111 patients were recorded during structured survey interviews. The experiences of healthcare professionals with the implementation process was recorded during 6 semi-structured interviews and 4 focus groups discussions (n = 27).
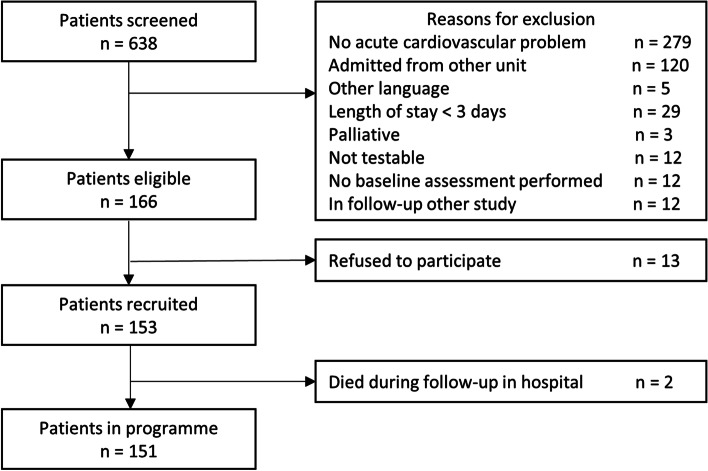
Results: The programme reached 91% in a sample of 151 patients with a mean age of 84 years. There was a high fidelity for the major components of the programme: documentation of geriatric risks (98%), co-management by specialist geriatrics nurse (95%), early rehabilitation (80%), and early discharge planning (74%), except for co-management by the geriatrician (32%). Both patients and healthcare professionals rated G-COACH as acceptable (95 and 94%) and feasible (96 and 74%). The healthcare professionals experienced staffing, competing roles and tasks of the geriatrics nurse and leadership support as important determinants for implementation.
Conclusions: The implementation strategy resulted in the successful initiation of the G-COACH programme. G-COACH was perceived as acceptable and feasible. Fidelity was influenced by context factors. Further investigation of the sustainability of the programme is needed.
Trial registration: ISRCTN22096382 (21/05/2020).
Keywords: Cardiovascular; Co-management; Frail; Geriatric; Geriatric assessment; Health services for the aged; Hospital; Implementation; Nursing.
© 2022. The Author(s).
Conflict of interest statement
The authors report no competing interests.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
