

Predictive value of circulating NMR metabolic biomarkers for type 2 diabetes risk in the UK Biobank study
- PMID: 35501852
- PMCID: PMC9063288
- DOI: 10.1186/s12916-022-02354-9
Predictive value of circulating NMR metabolic biomarkers for type 2 diabetes risk in the UK Biobank study
Abstract
Background: Effective targeted prevention of type 2 diabetes (T2D) depends on accurate prediction of disease risk. We assessed the role of metabolomic profiling in improving T2D risk prediction beyond conventional risk factors.
Methods: Nuclear magnetic resonance (NMR) metabolomic profiling was undertaken on baseline plasma samples in 65,684 UK Biobank participants without diabetes and not taking lipid-lowering medication. Among a subset of 50,519 participants with data available on all relevant co-variates (sociodemographic characteristics, parental history of diabetes, lifestyle-including dietary-factors, anthropometric measures and fasting time), Cox regression yielded adjusted hazard ratios for the associations of 143 individual metabolic biomarkers (including lipids, lipoproteins, fatty acids, amino acids, ketone bodies and other low molecular weight metabolic biomarkers) and 11 metabolic biomarker principal components (PCs) (accounting for 90% of the total variance in individual biomarkers) with incident T2D. These 11 PCs were added to established models for T2D risk prediction among the full study population, and measures of risk discrimination (c-statistic) and reclassification (continuous net reclassification improvement [NRI], integrated discrimination index [IDI]) were assessed.
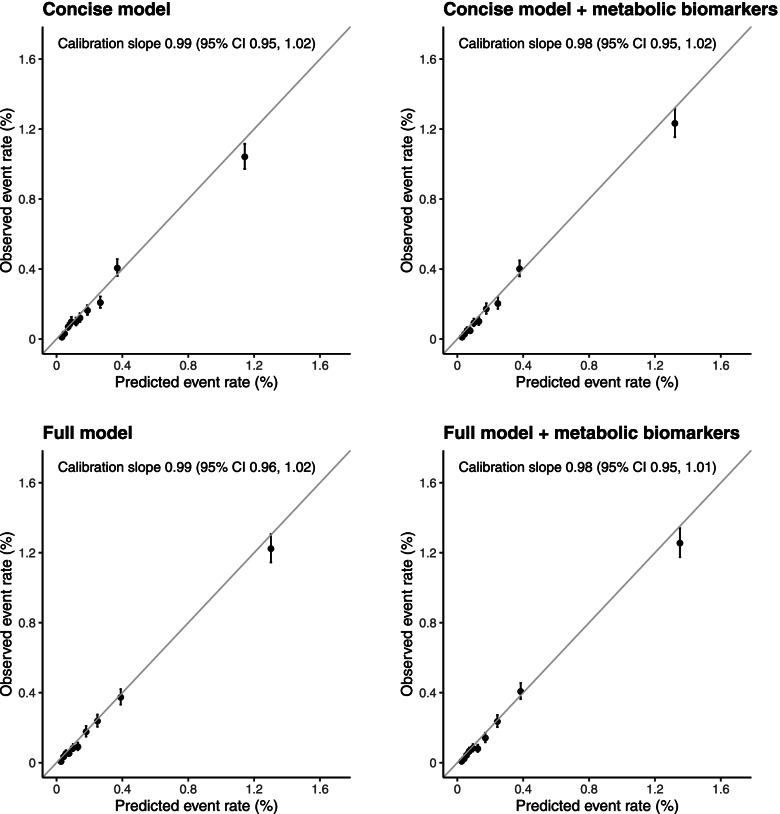
Results: During median 11.9 (IQR 11.1-12.6) years' follow-up, after accounting for multiple testing, 90 metabolic biomarkers showed independent associations with T2D risk among 50,519 participants (1211 incident T2D cases) and 76 showed associations after additional adjustment for HbA1c (false discovery rate controlled p < 0.01). Overall, 8 metabolic biomarker PCs were independently associated with T2D. Among the full study population of 65,684 participants, of whom 1719 developed T2D, addition of PCs to an established risk prediction model, including age, sex, parental history of diabetes, body mass index and HbA1c, improved T2D risk prediction as assessed by the c-statistic (increased from 0.802 [95% CI 0.791-0.812] to 0.830 [0.822-0.841]), continuous NRI (0.44 [0.38-0.49]) and relative (15.0% [10.5-20.4%]) and absolute (1.5 [1.0-1.9]) IDI. More modest improvements were observed when metabolic biomarker PCs were added to a more comprehensive established T2D risk prediction model additionally including waist circumference, blood pressure and plasma lipid concentrations (c-statistic, 0.829 [0.819-0.838] to 0.837 [0.831-0.848]; continuous NRI, 0.22 [0.17-0.28]; relative IDI, 6.3% [4.1-9.8%]; absolute IDI, 0.7 [0.4-1.1]).
Conclusions: When added to conventional risk factors, circulating NMR-based metabolic biomarkers modestly enhanced T2D risk prediction.
Keywords: Biomarkers; Diabetes; Metabolomics; Risk prediction.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Circulating metabolic biomarkers predict incident sepsis: a large-scale population study in the UK Biobank.Nutr J. 2025 Aug 15;24(1):126. doi: 10.1186/s12937-025-01191-9. Nutr J. 2025. PMID: 40817246 Free PMC article.
-
A cohort study reveals shared and distinct serum metabolic biomarkers for major adverse cardiovascular events in middle-aged and older adults.Geroscience. 2025 Feb 4. doi: 10.1007/s11357-025-01544-6. Online ahead of print. Geroscience. 2025. PMID: 39904969
-
The role of NMR-based circulating metabolic biomarkers in development and risk prediction of new onset type 2 diabetes.Sci Rep. 2022 Sep 5;12(1):15071. doi: 10.1038/s41598-022-19159-8. Sci Rep. 2022. PMID: 36064959 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Prognostic factors for the development and progression of proliferative diabetic retinopathy in people with diabetic retinopathy.Cochrane Database Syst Rev. 2023 Feb 22;2(2):CD013775. doi: 10.1002/14651858.CD013775.pub2. Cochrane Database Syst Rev. 2023. PMID: 36815723 Free PMC article. Review.
Cited by
-
The Paradoxical Role of Circulating Ketone Bodies in Glycemic Control of Individuals with Type 2 Diabetes: High Risk, High Reward?Biomolecules. 2022 Sep 18;12(9):1318. doi: 10.3390/biom12091318. Biomolecules. 2022. PMID: 36139157 Free PMC article.
-
Adults prenatally exposed to the Dutch Famine exhibit a metabolic signature associated with a broad spectrum of common diseases.BMC Med. 2024 Jul 29;22(1):309. doi: 10.1186/s12916-024-03529-2. BMC Med. 2024. PMID: 39075494 Free PMC article.
-
Novel type 2 diabetes prediction score based on traditional risk factors and circulating metabolites: model derivation and validation in two large cohort studies.EClinicalMedicine. 2024 Dec 6;79:102971. doi: 10.1016/j.eclinm.2024.102971. eCollection 2025 Jan. EClinicalMedicine. 2024. PMID: 39720612 Free PMC article.
-
Association of circulating metabolic biomarkers with risk of lung cancer: a population-based prospective cohort study.BMC Med. 2025 Mar 26;23(1):176. doi: 10.1186/s12916-025-03993-4. BMC Med. 2025. PMID: 40140895 Free PMC article.
-
Assessing the importance of primary care diagnoses in the UK Biobank.Eur J Epidemiol. 2024 Feb;39(2):219-229. doi: 10.1007/s10654-023-01095-0. Epub 2024 Jan 16. Eur J Epidemiol. 2024. PMID: 38225527 Free PMC article.
References
-
- Gillies CL, Abrams KR, Lambert PC, Cooper NJ, Sutton AJ, Hsu RT, et al. Pharmacological and lifestyle interventions to prevent or delay type 2 diabetes in people with impaired glucose tolerance: systematic review and meta-analysis. BMJ. 2007;334(7588):299. doi: 10.1136/bmj.39063.689375.55. - DOI - PMC - PubMed
-
- Gong Q, Zhang P, Wang J, Ma J, An Y, Chen Y, et al. Morbidity and mortality after lifestyle intervention for people with impaired glucose tolerance: 30-year results of the Da Qing diabetes prevention outcome study. Lancet Diabetes Endocrinol. 2019;7(6):452–461. doi: 10.1016/S2213-8587(19)30093-2. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
