

Involvement of IL-26 in bronchiolitis obliterans syndrome but not in acute rejection after lung transplantation
- PMID: 35501858
- PMCID: PMC9063324
- DOI: 10.1186/s12931-022-02036-3
Involvement of IL-26 in bronchiolitis obliterans syndrome but not in acute rejection after lung transplantation
Abstract
Background: The main long-term complication after lung transplantation is bronchiolitis obliterans syndrome (BOS), a deadly condition in which neutrophils may play a critical pathophysiological role. Recent studies show that the cytokine interleukin IL-26 can facilitate neutrophil recruitment in response to pro-inflammatory stimuli in the airways. In this pilot study, we characterized the local involvement of IL-26 during BOS and acute rejection (AR) in human patients.
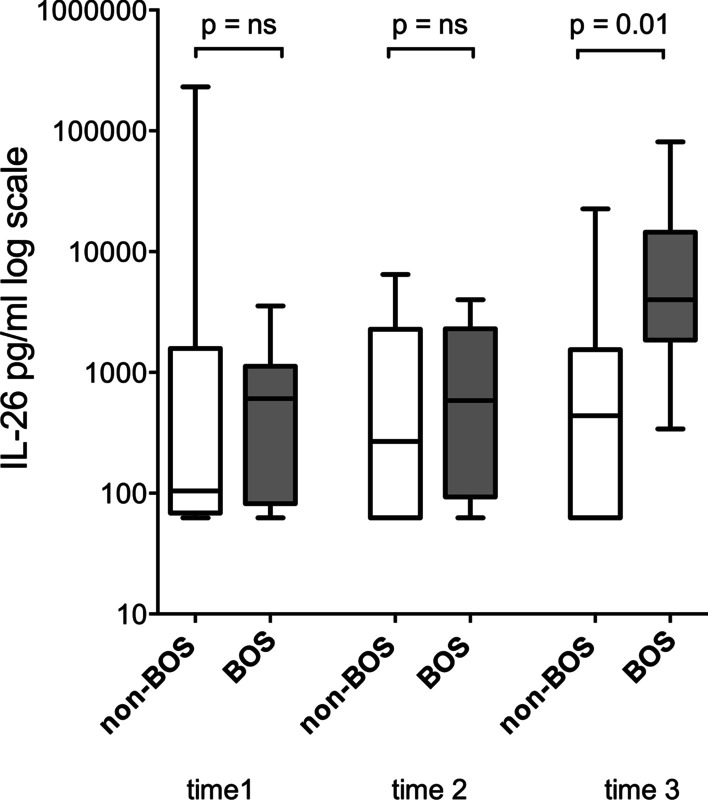
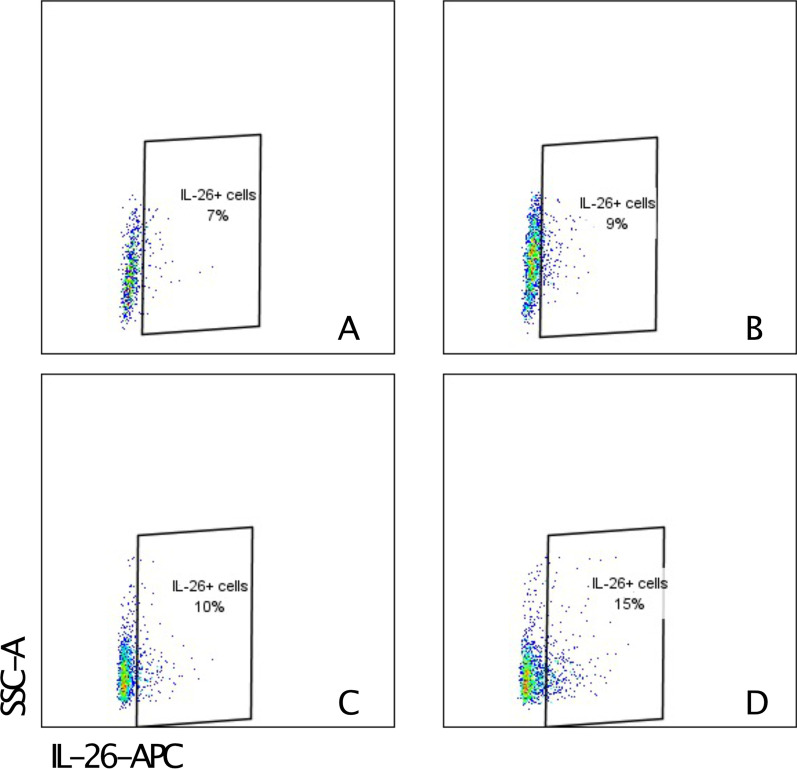
Method: From a biobank containing bronchoalveolar lavage (BAL) samples from 148 lung transplant recipients (LTR), clinically-matched patient pairs were identified to minimize the influence of clinical confounders. We identified ten pairs (BOS/non-BOS) with BAL samples harvested on three occasions for our longitudinal investigation and 12 pairs of patients with and without AR. The pairs were matched for age, gender, preoperative diagnosis, type of and time after surgery. Extracellular IL-26 protein was quantified in cell-free BAL samples using an enzyme-linked immunosorbent assay. Intracellular IL-26 protein in BAL cells was determined using immunocytochemistry (ICC) and flow cytometry.
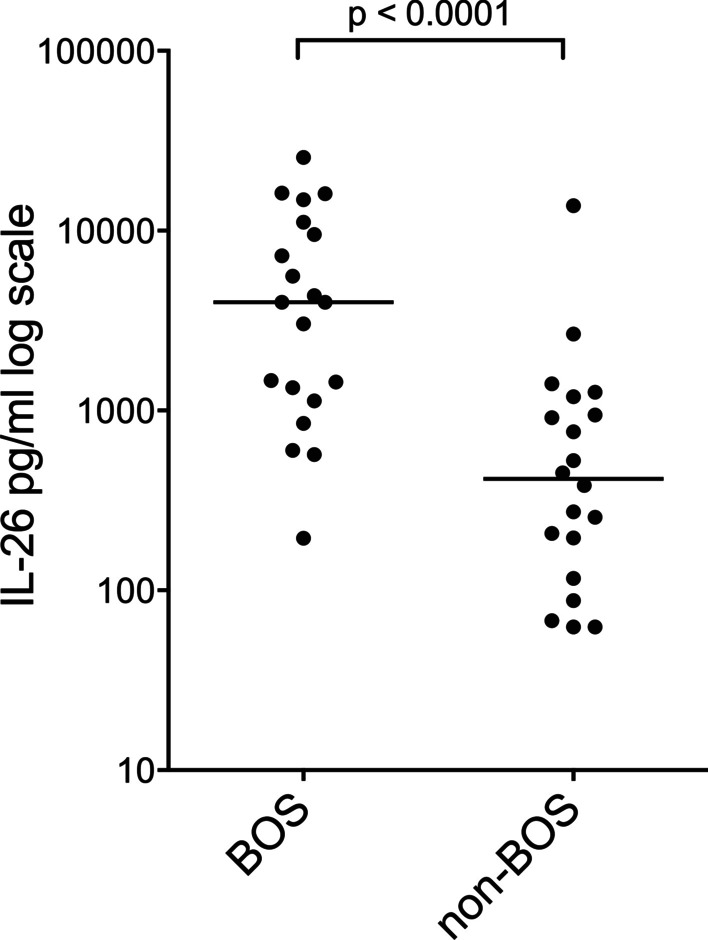
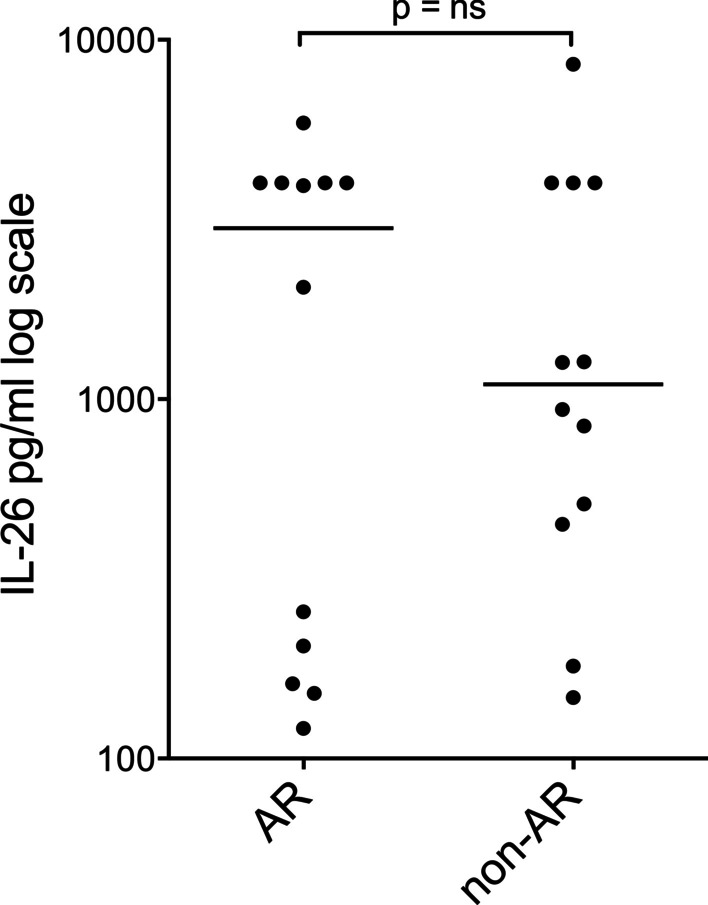
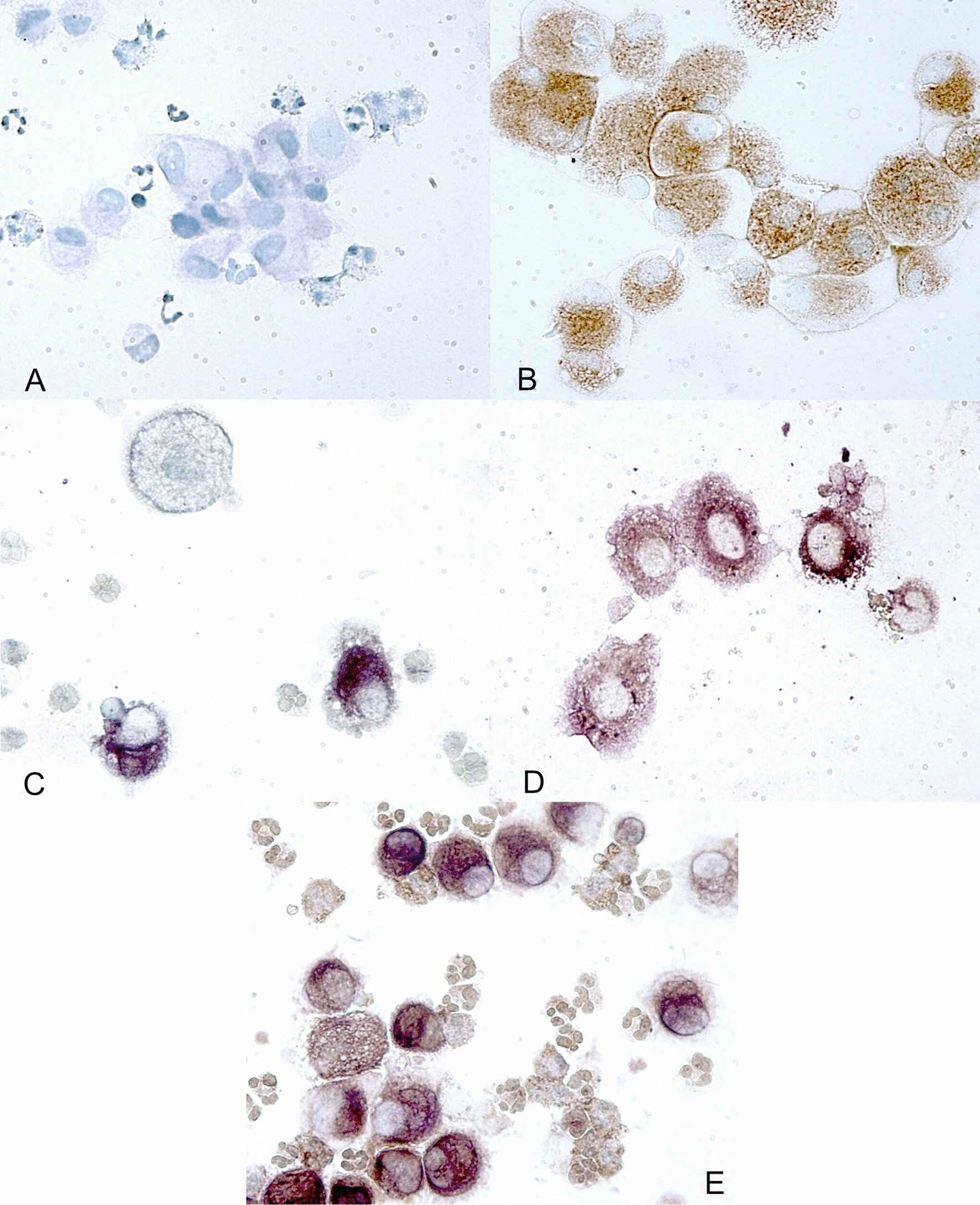
Results: The median extracellular concentration of IL-26 protein was markedly increased in BAL samples from patients with BOS (p < 0.0001) but not in samples from patients with AR. Intracellular IL-26 protein was confirmed in alveolar macrophages and lymphocytes (through ICC and flow cytometry) among BAL cells obtained from BOS patients.
Conclusions: Local IL-26 seems to be involved in BOS but not AR, and macrophages as well as lymphocytes constitute cellular sources in this clinical setting. The enhancement of extracellular IL-26 protein in LTRs with BOS warrants further investigation of its potential as a target for diagnosing, monitoring, and treating BOS.
Keywords: Acute rejection; Bronchiolitis obliterans syndrome; Cytokine; Interleukin-26; Lung transplantation; Neutrophil.
© 2022. The Author(s).
Conflict of interest statement
The authors have no financial relationship or conflict of interest associated with the contents of this manuscript.
Figures
References
-
- Cooper JD, Billingham M, Egan T, et al. A working formulation for the standardization of nomenclature and for clinical staging of chronic dysfunction in lung allografts. International Society for Heart and Lung Transplantation. J Heart Lung Transplant. 1993;12(5):713–716. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
