

Development and validation of qualitative and quantitative models to predict invasiveness of lung adenocarcinomas manifesting as pure ground-glass nodules based on low-dose computed tomography during lung cancer screening
- PMID: 35502397
- PMCID: PMC9014141
- DOI: 10.21037/qims-21-912
Development and validation of qualitative and quantitative models to predict invasiveness of lung adenocarcinomas manifesting as pure ground-glass nodules based on low-dose computed tomography during lung cancer screening
Abstract
Background: Due to different management strategy and prognosis of different subtypes of lung adenocarcinomas appearing as pure ground-glass nodules (pGGNs), it is important to differentiate invasive adenocarcinoma (IA) from adenocarcinoma in situ/minimally invasive adenocarcinoma (AIS/MIA) during lung cancer screening. The aim of this study was to develop and validate the qualitative and quantitative models to predict the invasiveness of lung adenocarcinoma appearing as pGGNs based on low-dose computed tomography (LDCT) and compare their diagnostic performance with that of intraoperative frozen section (FS).
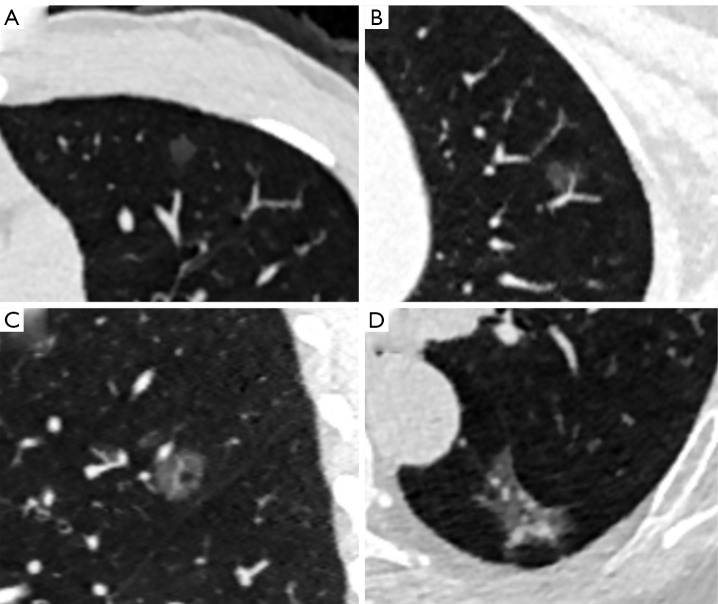
Methods: A total of 223 consecutive pathologically confirmed pGGNs from March 2018 to December 2020 were divided into a primary cohort (96 IAs and 64 AIS/MIAs) and validation cohort (39 IAs and 24 AIS/MIAs) according to scans (Brilliance iCT and Somatom Definition Flash) performed at Sichuan Cancer Hospital and Institute. The following LDCT features of pGGNs were analyzed: the qualitative features included nodule location, shape, margin, nodule-lung interface, lobulation, spiculation, pleural indentation, air bronchogram, vacuole, and vessel type, and the quantitative features included the diameter, volume, and mean attenuation. Multivariate logistic regression analysis was used to build a qualitative model, quantitative model, and combined qualitative and quantitative model. The diagnostic performance was assessed according to the following factors: the area under curve (AUC) of the receiver operating characteristic (ROC) curve, sensitivity, specificity, and accuracy.
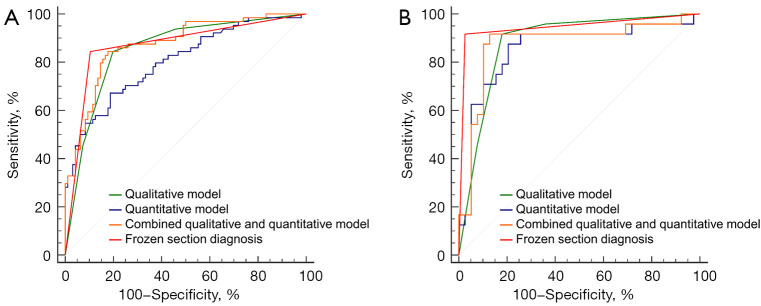
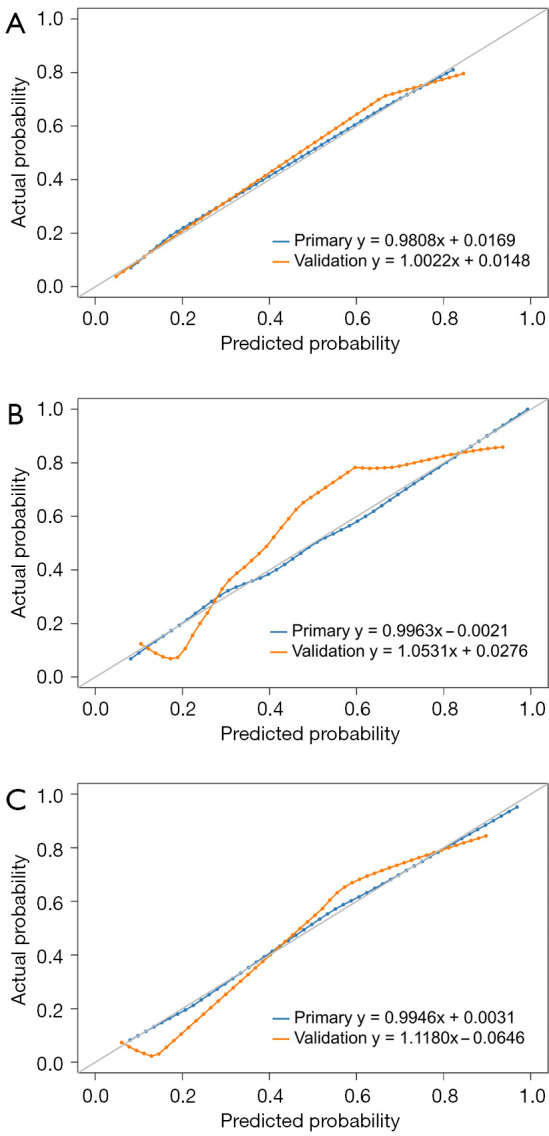
Results: The AUCs of the qualitative model, quantitative model, combined qualitative and quantitative model, and the FS diagnosis were 0.854, 0.803, 0.873, and 0.870, respectively, in the primary cohort and 0.884, 0.855, 0.875, and 0.946, respectively, in the validation cohort. No significant difference of the AUCs was found among the radiological models and the FS diagnosis in the primary or validation cohort (all corrected P>0.05). Among the radiological models, the combined qualitative and quantitative model consisting of vessel type and volume showed the highest accuracy in both the primary and validation cohorts (0.831 and 0.889, respectively).
Conclusions: The diagnostic performances of the qualitative and quantitative models based on LDCT to differentiate IA from AIS/MIA in pGGNs are equivalent to that of intraoperative FS diagnosis. The vessel type and volume can be preoperative and non-invasive biomarkers to assess the invasive risk of pGGNs in lung cancer screening.
Keywords: Pure ground-glass nodule (pGGN); low-dose computed tomography (LDCT); lung adenocarcinoma; lung cancer screening.
2022 Quantitative Imaging in Medicine and Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-21-912/coif). The authors have no conflicts of interest to declare.
Figures
References
-
- Aberle DR, DeMello S, Berg CD, Black WC, Brewer B, Church TR, Clingan KL, Duan F, Fagerstrom RM, Gareen IF, Gatsonis CA, Gierada DS, Jain A, Jones GC, Mahon I, Marcus PM, Rathmell JM, Sicks J, National Lung Screening Trial Research Team . Results of the two incidence screenings in the National Lung Screening Trial. N Engl J Med 2013;369:920-31. 10.1056/NEJMoa1208962 - DOI - PMC - PubMed
-
- Patz EF, Jr, Greco E, Gatsonis C, Pinsky P, Kramer BS, Aberle DR. Lung cancer incidence and mortality in National Lung Screening Trial participants who underwent low-dose CT prevalence screening: a retrospective cohort analysis of a randomised, multicentre, diagnostic screening trial. Lancet Oncol 2016;17:590-9. 10.1016/S1470-2045(15)00621-X - DOI - PMC - PubMed
-
- Wang Z, Han W, Zhang W, Xue F, Wang Y, Hu Y, Wang L, Zhou C, Huang Y, Zhao S, Song W, Sui X, Shi R, Jiang J. Mortality outcomes of low-dose computed tomography screening for lung cancer in urban China: a decision analysis and implications for practice. Chin J Cancer 2017;36:57. 10.1186/s40880-017-0221-8 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources