

Postprandial symptoms in patients with symptoms of gastroparesis: roles of gastric emptying and accommodation
- PMID: 35502871
- PMCID: PMC9236865
- DOI: 10.1152/ajpgi.00278.2021
Postprandial symptoms in patients with symptoms of gastroparesis: roles of gastric emptying and accommodation
Abstract
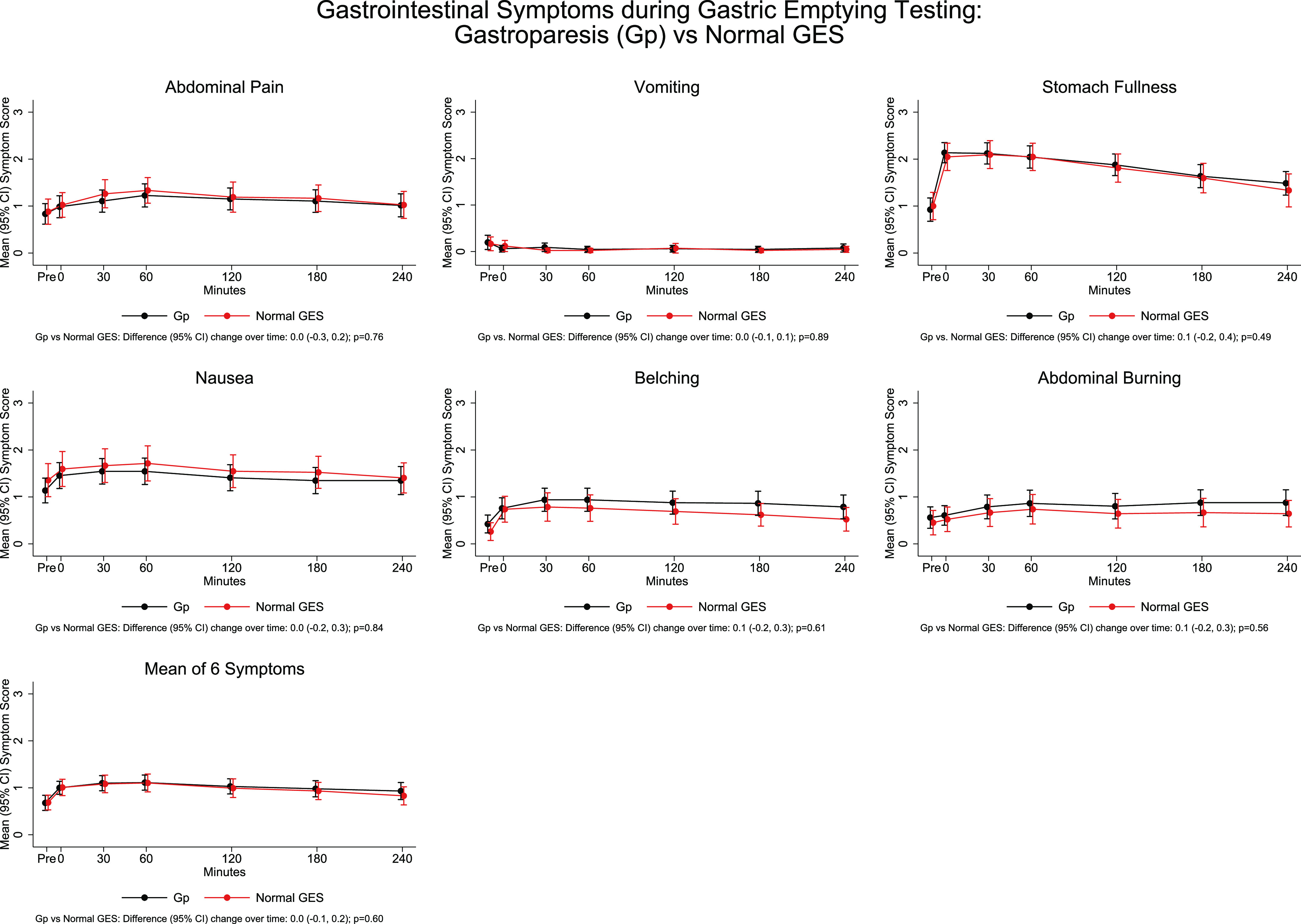
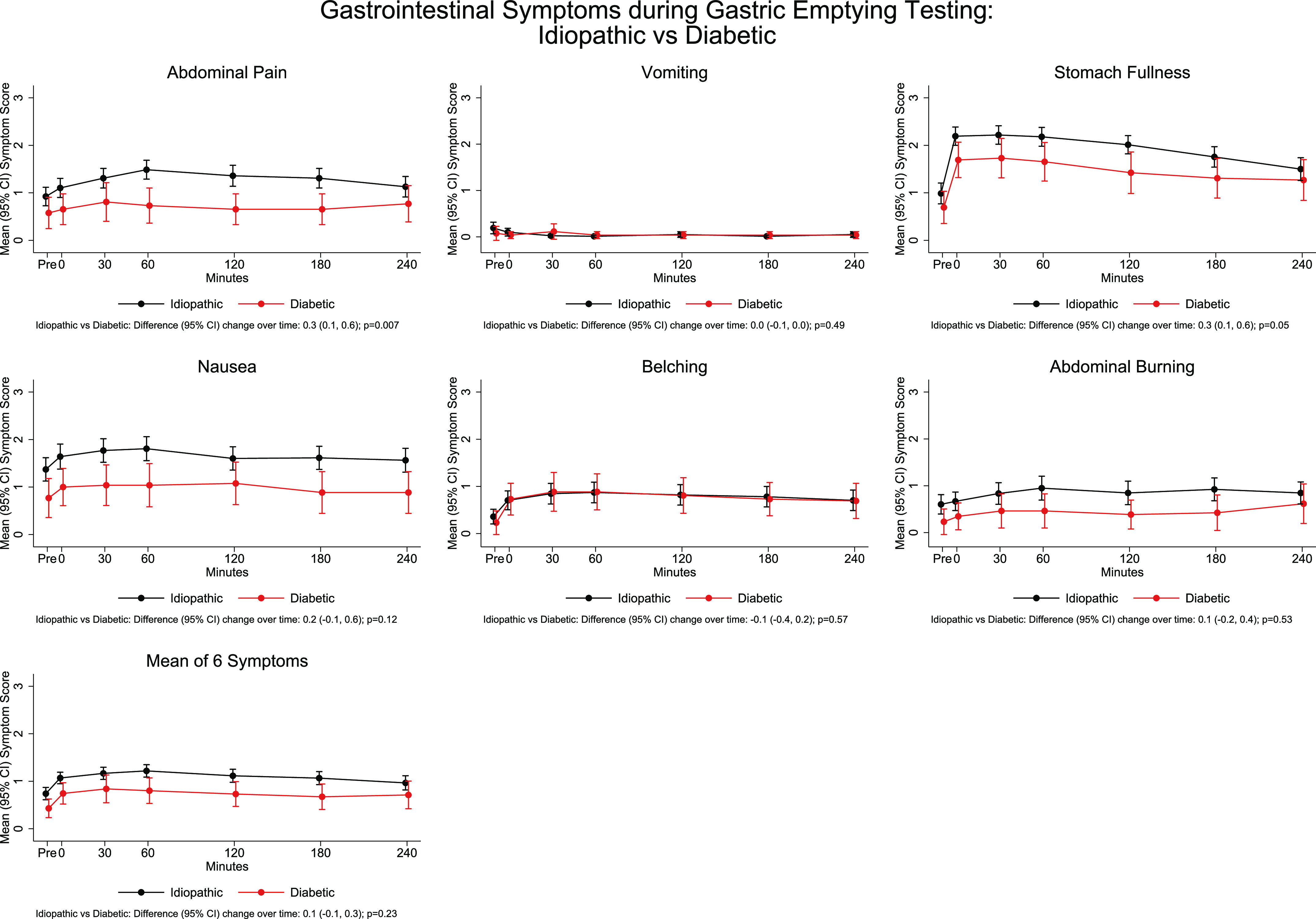
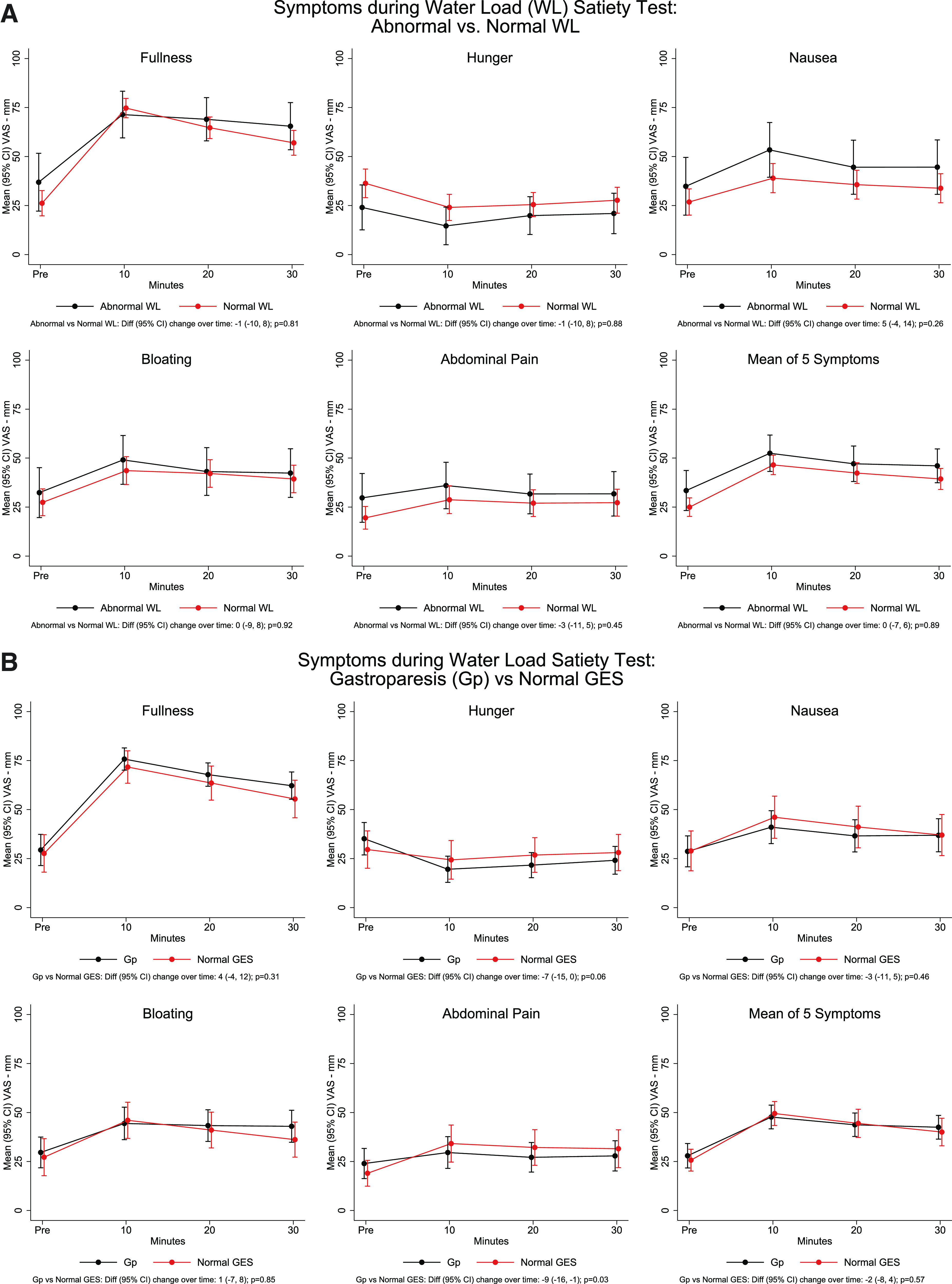
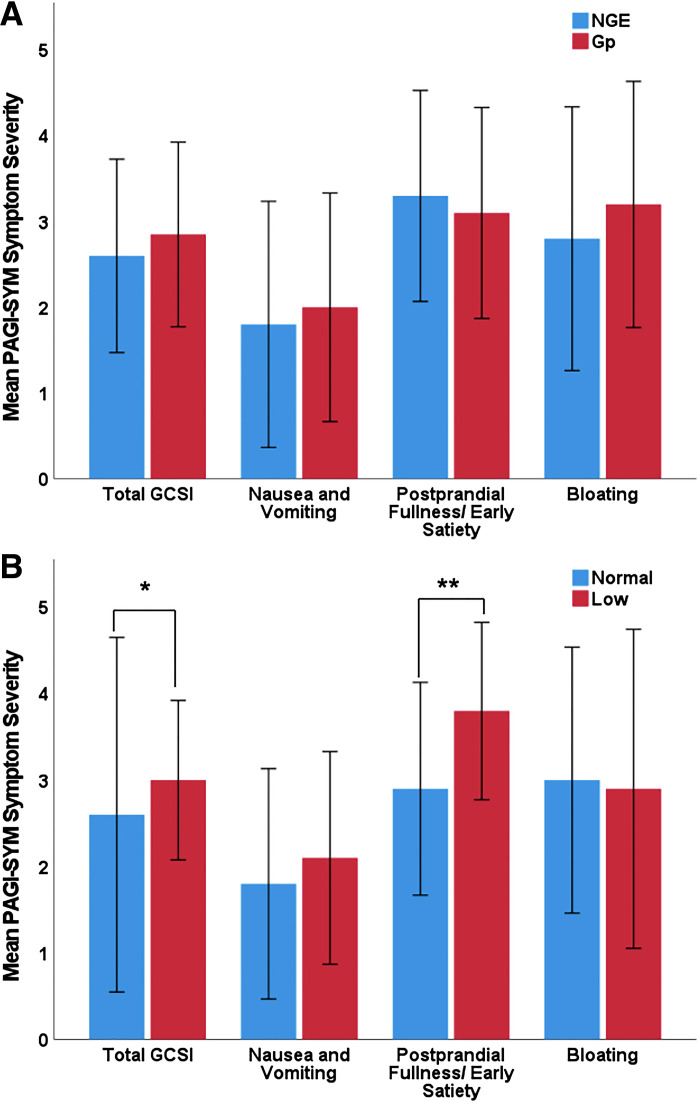
Patients often are evaluated for gastroparesis because of symptoms occurring with meals. Gastric emptying scintigraphy (GES) is used for gastroparesis diagnosis, although results are not well correlated with gastroparesis symptoms. The aim of this study is to assess relationships between gastroparesis symptoms, gastric emptying (GE), and gastric accommodation (GA). Patients with symptoms of gastroparesis completed the Patient Assessment of Upper GI Symptoms (PAGI-SYM) and recorded symptoms during GES and water load satiety test (WLST), an indirect assessment for GA. A total of 109 patients with gastroparesis symptoms were assessed. Symptom severity increased after GES meal for stomach fullness, belching, nausea, abdominal burning, and abdominal pain. There was no difference in symptoms after meal between patients with delayed (n = 66) and normal (n = 42) GE. Diabetic patients (n = 26) had greater gastric retention than idiopathic patients (n = 78), but idiopathic patients had greater postprandial nausea, stomach fullness, and abdominal pain. Water consumed during WLST averaged 421 ± 245 mL. Idiopathic patients had greater nausea scores during WLST than diabetic patients. In comparison to those with normal water consumption (≥238 mL; n = 80), patients with impaired water ingestion (<238 mL; n = 26) had increased stomach fullness, early satiety, postprandial fullness, and loss of appetite on PAGI-SYM. Patients with delayed and normal GE had similar symptom profiles during GES and WLST. Idiopathic patients had less gastric retention but more symptoms after GES meal and after WLST compared with diabetic patients. Patients with impaired water consumption during WLST had increased symptoms by PAGI-SYM. These data suggest that impaired GA, rather than GE, may be important in explaining postprandial symptoms in patients with symptoms of gastroparesis.NEW & NOTEWORTHY Patients with delayed and normal gastric emptying (GE) had similar symptom profiles during gastric emptying scintigraphy (GES). Idiopathic patients with symptoms of gastroparesis had less gastric retention by GES; but more symptoms after GES meal and after water load satiety test (WLST) compared with diabetic patients. In patients with symptoms of gastroparesis, symptoms after WLST increased with decreasing water consumption. Early satiety and loss of appetite were associated with decreased water consumption during WLST. Thus, impaired accommodation and perhaps visceral hypersensitivity are important in explaining postprandial symptoms in gastroparesis.
Trial registration: ClinicalTrials.gov NCT01696747.
Keywords: gastric accommodation; gastric emptying; gastroparesis.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures

References
-
- Pasricha PJ, Colvin R, Yates K, Hasler WL, Abell TL, Unalp-Arida A, Nguyen L, Farrugia G, Koch KL, Parkman HP, Snape WJ, Lee L, Tonascia J, Hamilton F. Characteristics of patients with chronic unexplained nausea and vomiting and normal gastric emptying. Clin Gastroenterol Hepatol 9: 567–576, 2011. doi: 10.1016/j.cgh.2011.03.003. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical