

Sex-Specific Risk Factors Associated With First Acute Myocardial Infarction in Young Adults
- PMID: 35503221
- PMCID: PMC9066284
- DOI: 10.1001/jamanetworkopen.2022.9953
Sex-Specific Risk Factors Associated With First Acute Myocardial Infarction in Young Adults
Abstract
Importance: An increasing proportion of people in the US hospitalized for acute myocardial infarction (AMI) are younger than 55 years, with the largest increase in young women. Effective prevention requires an understanding of risk factors associated with risk of AMI in young women compared with men.
Objectives: To assess the sex-specific associations of demographic, clinical, and psychosocial risk factors with first AMI among adults younger than 55 years, overall, and by AMI subtype.
Design, setting, and participants: This study used a case-control design with 2264 patients with AMI, aged 18 to 55 years, from the VIRGO (Variation in Recovery: Role of Gender on Outcomes of Young AMI Patients) study and 2264 population-based controls matched for age, sex, and race and ethnicity from the National Health and Nutrition Examination Survey from 2008 to 2012. Data were analyzed from April 2020 to November 2021.
Exposures: A wide range of demographic, clinical, and psychosocial risk factors.
Main outcomes and measures: Odds ratios (ORs) and population attributable fractions (PAF) for first AMI associated with demographic, clinical, and psychosocial risk factors.
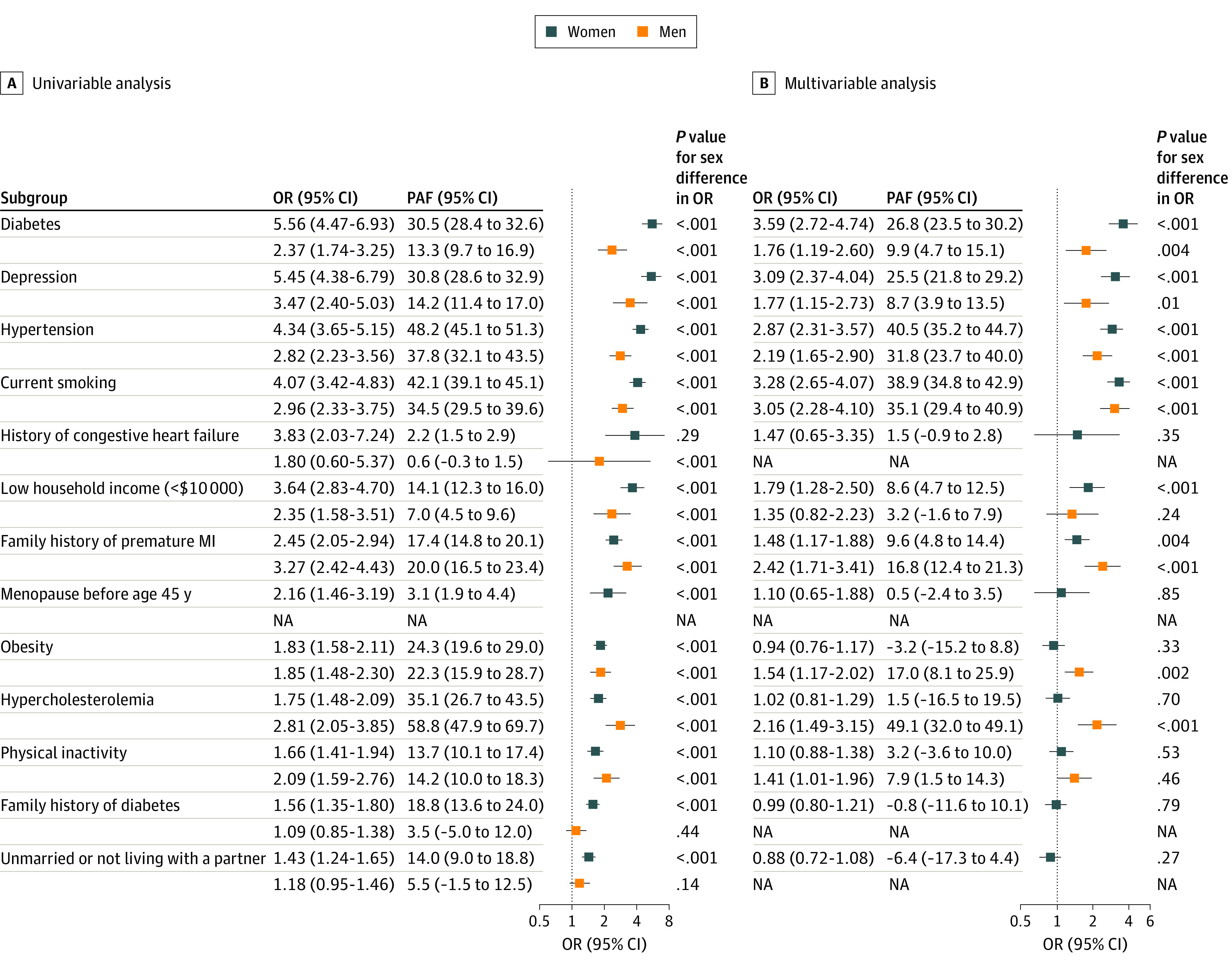
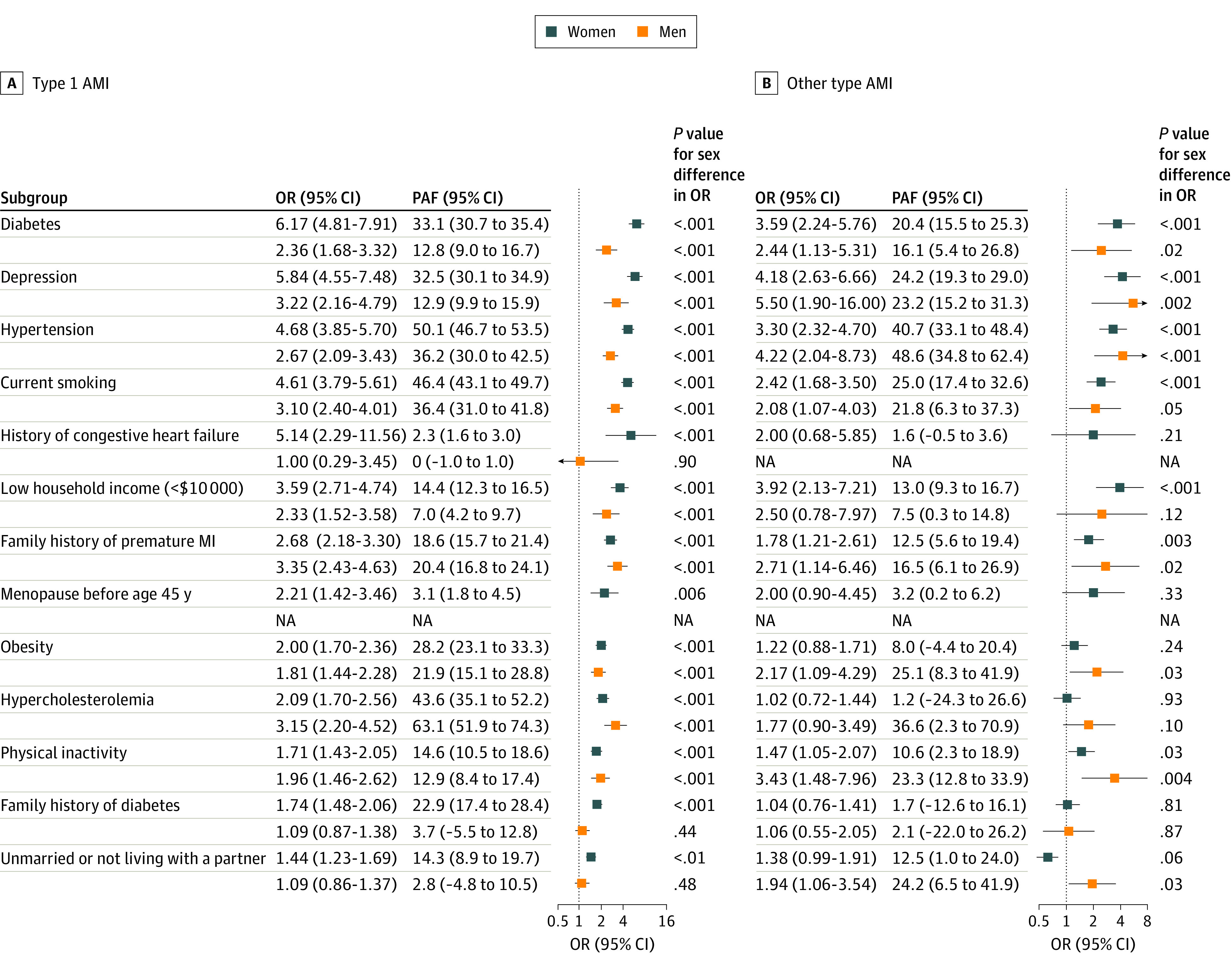
Results: Of the 4528 case patients and matched controls, 3122 (68.9%) were women, and the median (IQR) age was 48 (44-52) years. Seven risk factors (diabetes [OR, 3.59 (95% CI, 2.72-4.74) in women vs 1.76 (1.19-2.60) in men], depression [OR, 3.09 (95% CI, 2.37-4.04) in women vs 1.77 (1.15-2.73) in men], hypertension [OR, 2.87 (95% CI, 2.31-3.57) in women vs 2.19 (1.65-2.90) in men], current smoking [OR, 3.28 (95% CI, 2.65-4.07) in women vs 3.28 (2.65-4.07) in men], family history of premature myocardial infarction [OR, 1.48 (95% CI, 1.17-1.88) in women vs 2.42 (1.71-3.41) in men], low household income [OR, 1.79 (95% CI, 1.28-2.50) in women vs 1.35 (0.82-2.23) in men], hypercholesterolemia [OR, 1.02 (95% CI, 0.81-1.29) in women vs 2.16 (1.49-3.15) in men]) collectively accounted for the majority of the total risk of AMI in women (83.9%) and men (85.1%). There were significant sex differences in risk factor associations: hypertension, depression, diabetes, current smoking, and family history of diabetes had stronger associations with AMI in young women, whereas hypercholesterolemia had a stronger association in young men. Risk factor profiles varied by AMI subtype, and traditional cardiovascular risk factors had higher prevalence and stronger ORs for type 1 AMI compared with other AMI subtypes.
Conclusions and relevance: In this case-control study, 7 risk factors, many potentially modifiable, accounted for 85% of the risk of first AMI in young women and men. Significant differences in risk factor profiles and risk factor associations existed by sex and by AMI subtype. These findings suggest the need for sex-specific strategies in risk factor modification and prevention of AMI in young adults. Further research is needed to improve risk assessment of AMI subtypes.
Conflict of interest statement
Figures
References
-
- Benjamin EJ, Virani SS, Callaway CW, et al. ; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee . Heart disease and stroke statistics—2018 update: a report from the American Heart Association. Circulation. 2018;137(12):e67-e492. doi: 10.1161/CIR.0000000000000558 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
