

Effect of Self-monitoring of Blood Pressure on Blood Pressure Control in Pregnant Individuals With Chronic or Gestational Hypertension: The BUMP 2 Randomized Clinical Trial
- PMID: 35503345
- PMCID: PMC9066282
- DOI: 10.1001/jama.2022.4726
Effect of Self-monitoring of Blood Pressure on Blood Pressure Control in Pregnant Individuals With Chronic or Gestational Hypertension: The BUMP 2 Randomized Clinical Trial
Abstract
Importance: Inadequate management of elevated blood pressure is a significant contributing factor to maternal deaths. The role of blood pressure self-monitoring in pregnancy in improving clinical outcomes for the pregnant individual and infant is unclear.
Objective: To evaluate the effect of blood pressure self-monitoring, compared with usual care alone, on blood pressure control and other related maternal and infant outcomes, in individuals with pregnancy hypertension.
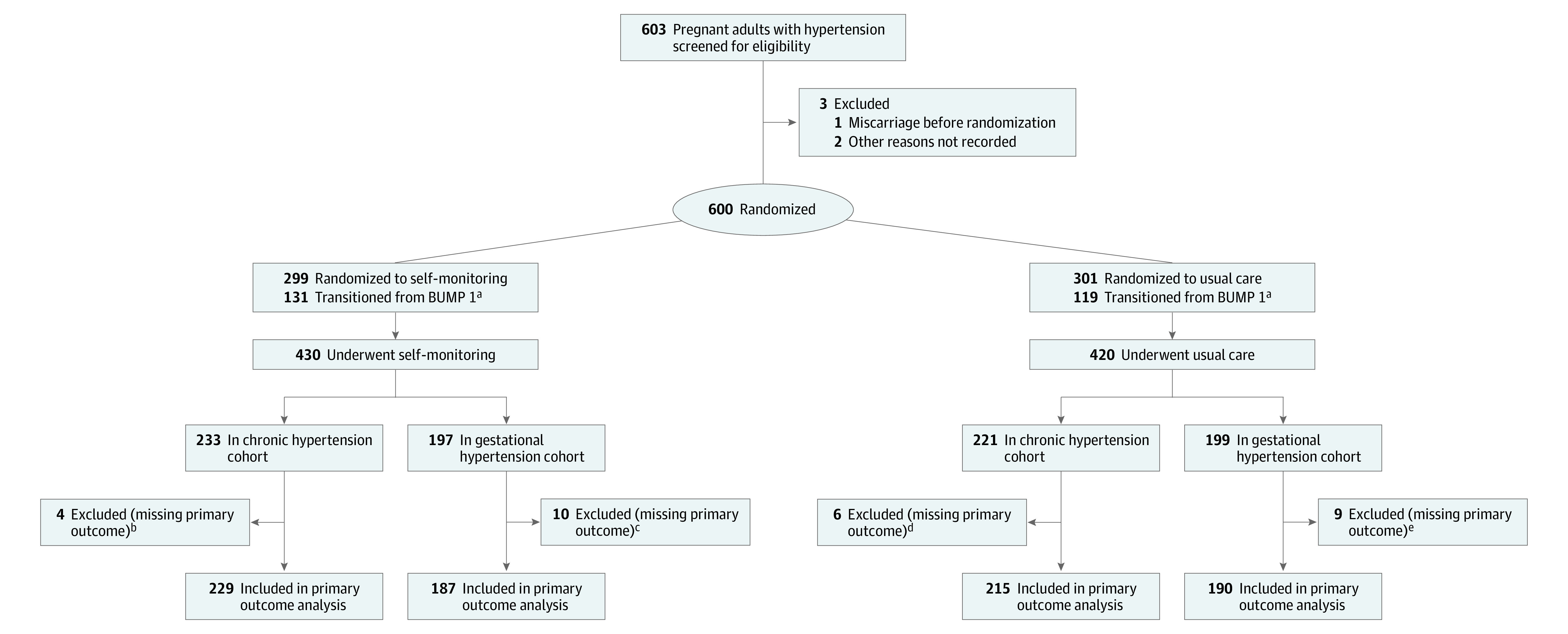
Design, setting, and participants: Unblinded, randomized clinical trial that recruited between November 2018 and September 2019 in 15 hospital maternity units in England. Individuals with chronic hypertension (enrolled up to 37 weeks' gestation) or with gestational hypertension (enrolled between 20 and 37 weeks' gestation). Final follow-up was in May 2020.
Interventions: Participants were randomized to either blood pressure self-monitoring using a validated monitor and a secure telemonitoring system in addition to usual care (n = 430) or to usual care alone (n = 420). Usual care comprised blood pressure measured by health care professionals at regular antenatal clinics.
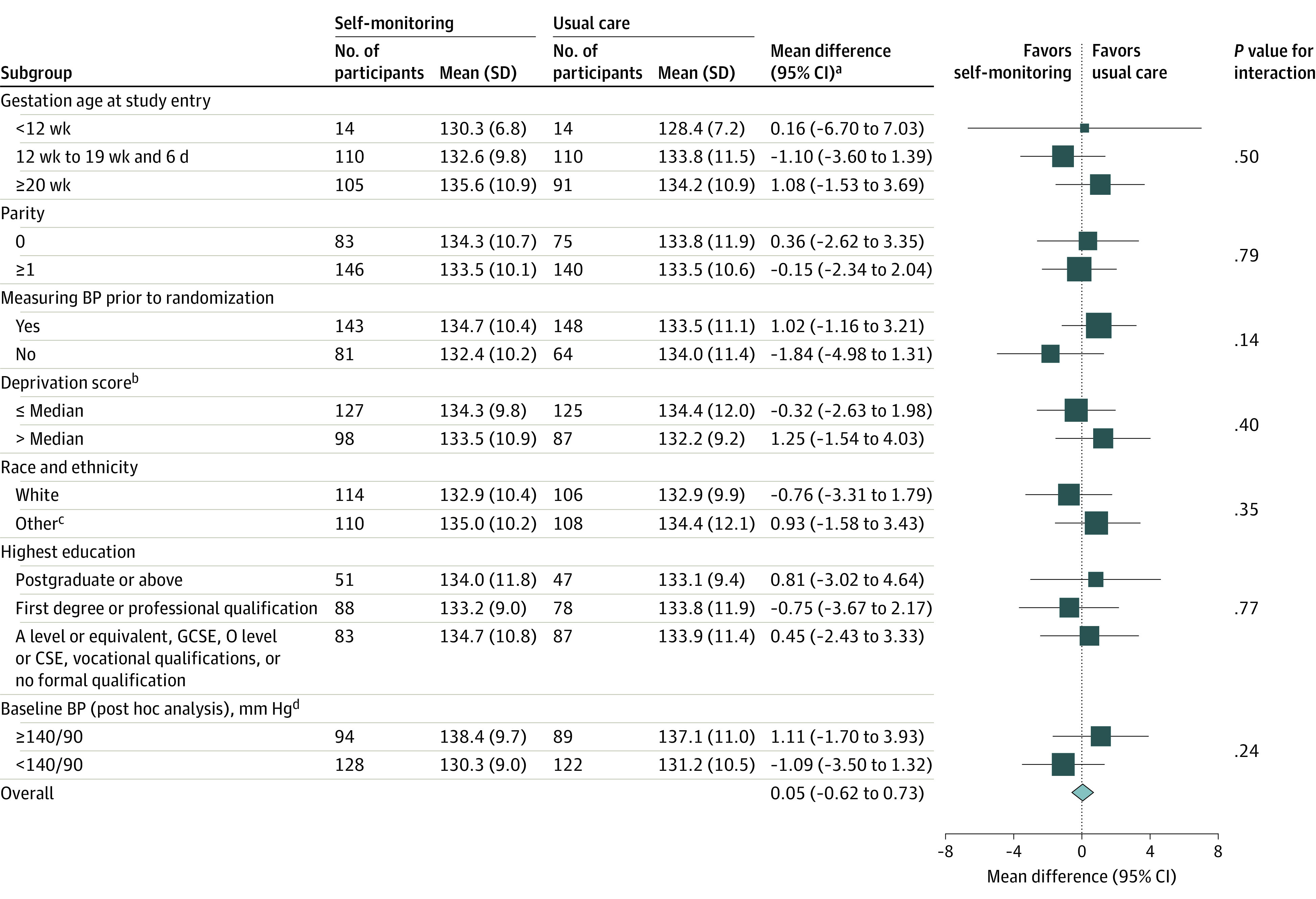
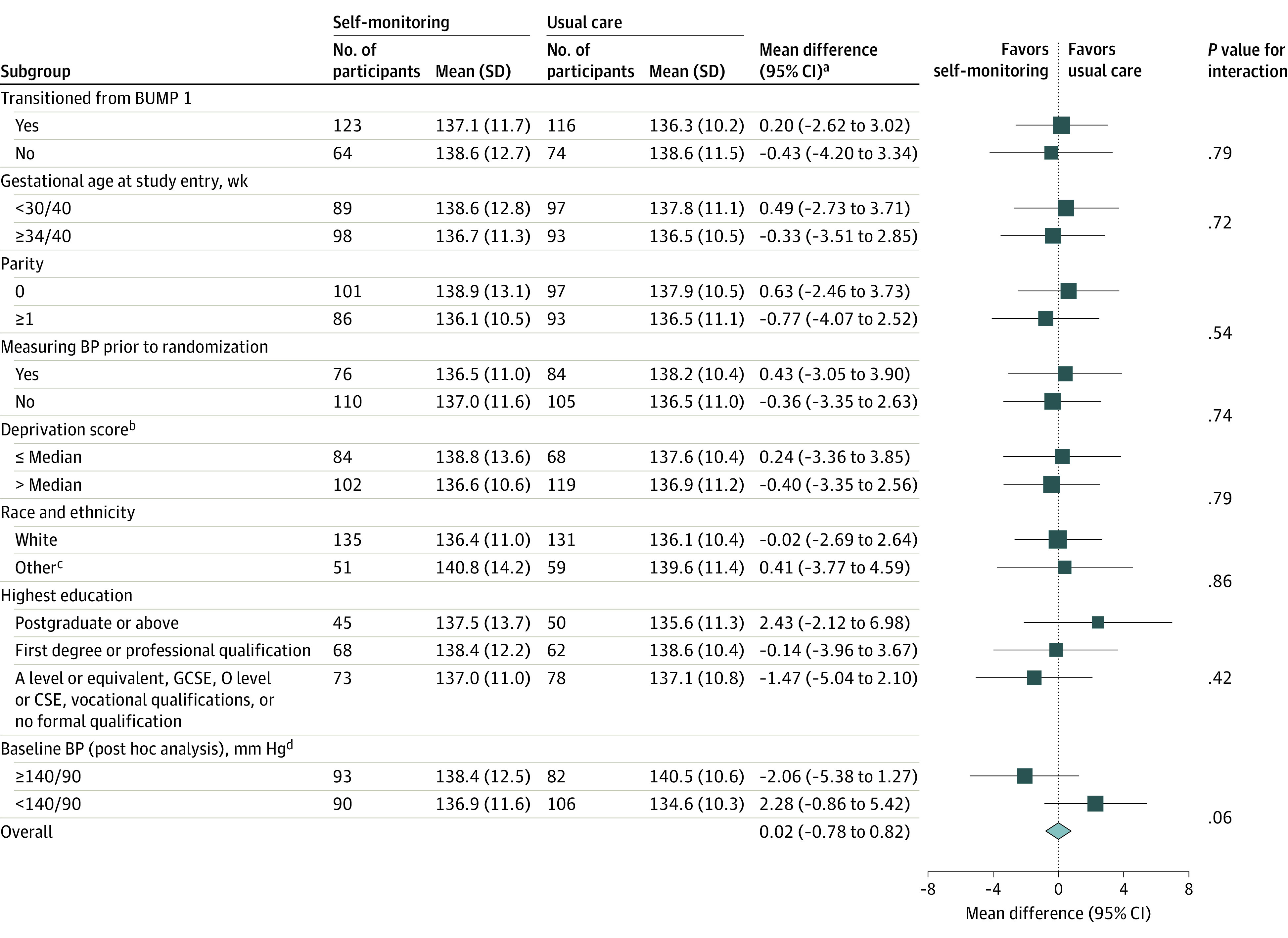
Main outcomes and measures: The primary maternal outcome was the difference in mean systolic blood pressure recorded by health care professionals between randomization and birth.
Results: Among 454 participants with chronic hypertension (mean age, 36 years; mean gestation at entry, 20 weeks) and 396 with gestational hypertension (mean age, 34 years; mean gestation at entry, 33 weeks) who were randomized, primary outcome data were available from 444 (97.8%) and 377 (95.2%), respectively. In the chronic hypertension cohort, there was no statistically significant difference in mean systolic blood pressure for the self-monitoring groups vs the usual care group (133.8 mm Hg vs 133.6 mm Hg, respectively; adjusted mean difference, 0.03 mm Hg [95% CI, -1.73 to 1.79]). In the gestational hypertension cohort, there was also no significant difference in mean systolic blood pressure (137.6 mm Hg compared with 137.2 mm Hg; adjusted mean difference, -0.03 mm Hg [95% CI, -2.29 to 2.24]). There were 8 serious adverse events in the self-monitoring group (4 in each cohort) and 3 in the usual care group (2 in the chronic hypertension cohort and 1 in the gestational hypertension cohort).
Conclusions and relevance: Among pregnant individuals with chronic or gestational hypertension, blood pressure self-monitoring with telemonitoring, compared with usual care, did not lead to significantly improved clinic-based blood pressure control.
Trial registration: ClinicalTrials.gov Identifier: NCT03334149.
Conflict of interest statement
Figures
Comment in
-
Self-monitoring of Blood Pressure During Pregnancy.JAMA. 2022 May 3;327(17):1651-1652. doi: 10.1001/jama.2022.2802. JAMA. 2022. PMID: 35503365 No abstract available.
