

Effect of Self-monitoring of Blood Pressure on Diagnosis of Hypertension During Higher-Risk Pregnancy: The BUMP 1 Randomized Clinical Trial
- PMID: 35503346
- PMCID: PMC9066279
- DOI: 10.1001/jama.2022.4712
Effect of Self-monitoring of Blood Pressure on Diagnosis of Hypertension During Higher-Risk Pregnancy: The BUMP 1 Randomized Clinical Trial
Erratum in
-
Data Errors in Table 1 of Blood Pressure Self-monitoring Trial.JAMA. 2022 Jul 12;328(2):217. doi: 10.1001/jama.2022.11186. JAMA. 2022. PMID: 35819441 Free PMC article. No abstract available.
Abstract
Importance: Inadequate management of elevated blood pressure (BP) is a significant contributing factor to maternal deaths. Self-monitoring of BP in the general population has been shown to improve the diagnosis and management of hypertension; however, little is known about its use in pregnancy.
Objective: To determine whether self-monitoring of BP in higher-risk pregnancies leads to earlier detection of pregnancy hypertension.
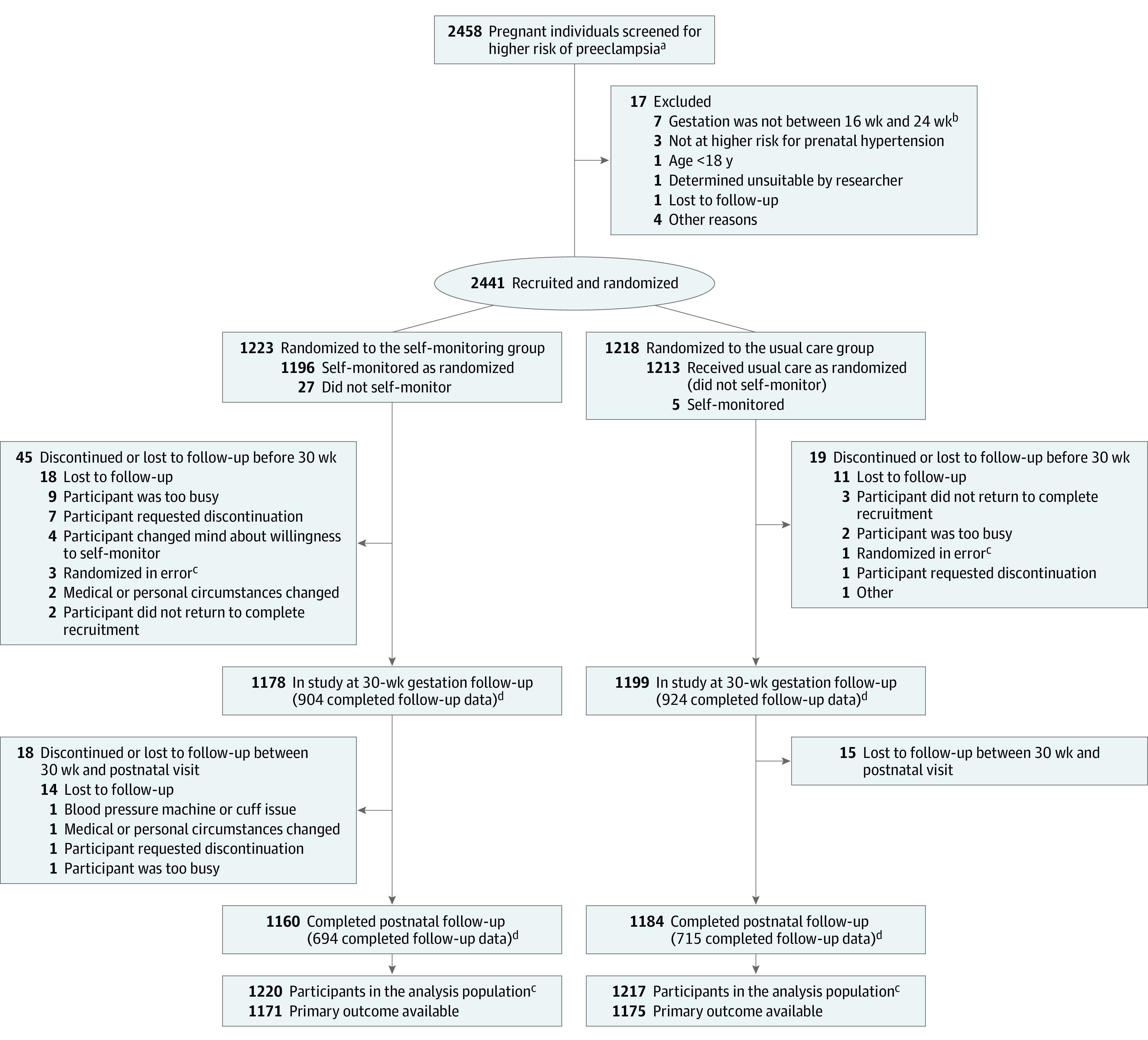
Design, setting, and participants: Unblinded, randomized clinical trial that included 2441 pregnant individuals at higher risk of preeclampsia and recruited at a mean of 20 weeks' gestation from 15 hospital maternity units in England between November 2018 and October 2019. Final follow-up was completed in April 2020.
Interventions: Participating individuals were randomized to either BP self-monitoring with telemonitoring (n = 1223) plus usual care or usual antenatal care alone (n = 1218) without access to telemonitored BP.
Main outcomes and measures: The primary outcome was time to first recorded hypertension measured by a health care professional.
Results: Among 2441 participants who were randomized (mean [SD] age, 33 [5.6] years; mean gestation, 20 [1.6] weeks), 2346 (96%) completed the trial. The time from randomization to clinic recording of hypertension was not significantly different between individuals in the self-monitoring group (mean [SD], 104.3 [32.6] days) vs in the usual care group (mean [SD], 106.2 [32.0] days) (mean difference, -1.6 days [95% CI, -8.1 to 4.9]; P = .64). Eighteen serious adverse events were reported during the trial with none judged as related to the intervention (12 [1%] in the self-monitoring group vs 6 [0.5%] in the usual care group).
Conclusions and relevance: Among pregnant individuals at higher risk of preeclampsia, blood pressure self-monitoring with telemonitoring, compared with usual care, did not lead to significantly earlier clinic-based detection of hypertension.
Trial registration: ClinicalTrials.gov Identifier: NCT03334149.
Conflict of interest statement
Figures
Comment in
-
Self-monitoring of Blood Pressure During Pregnancy.JAMA. 2022 May 3;327(17):1651-1652. doi: 10.1001/jama.2022.2802. JAMA. 2022. PMID: 35503365 No abstract available.
References
-
- Cantwell R, Clutton-Brock T, Cooper G, et al. Saving Mothers’ Lives: reviewing maternal deaths to make motherhood safer: 2006-2008. The Eighth Report of the Confidential Enquiries into Maternal Deaths in the United Kingdom. BJOG. 2011;118(suppl 1):1-203. doi: 10.1111/j.1471-0528.2010.02847.x - DOI - PubMed
-
- Saving Lives, Improving Mothers’ Care: Lessons Learned to Inform Maternity Care From the UK and Ireland: Confidential Enquiries Into Maternal Deaths and Morbidity 2016-18. University of Oxford; 2020.
-
- NICE . Hypertension in pregnancy: diagnosis and management (clinical guideline CG107). National Institute for Health and Care Excellence. August 25, 2010. Accessed February 8, 2022. https://www.nice.org.uk/guidance/cg107
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
