

Endovascular Therapy for Intracranial Giant Cell Arteritis : Systematic Review, Technical Considerations and the Effect of Intra-arterial Calcium Channel Blockers
- PMID: 35503467
- PMCID: PMC9744710
- DOI: 10.1007/s00062-022-01171-0
Endovascular Therapy for Intracranial Giant Cell Arteritis : Systematic Review, Technical Considerations and the Effect of Intra-arterial Calcium Channel Blockers
Abstract
Background: Giant cell arteritis (GCA) is a systemic vasculitis that may cause ischemic stroke. Rarely, GCA can present with aggressive intracranial stenoses, which are refractory to medical therapy. Endovascular treatment (EVT) is a possible rescue strategy to prevent ischemic complications in intracranial GCA but the safety and efficacy of EVT in this setting are not well-described.
Methods: A systematic literature review was performed to identify case reports and series with individual patient-level data describing EVT for intracranial GCA. The clinical course, therapeutic considerations, and technique of seven endovascular treatments in a single patient from the authors' experience are presented.
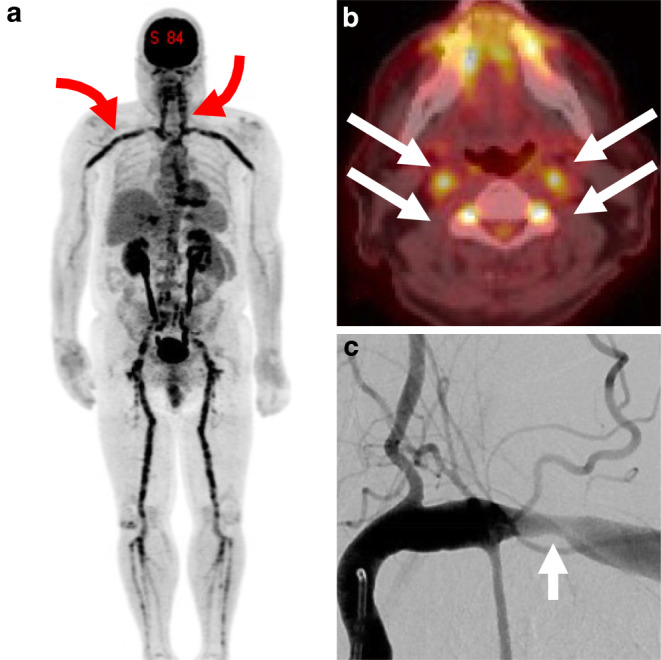
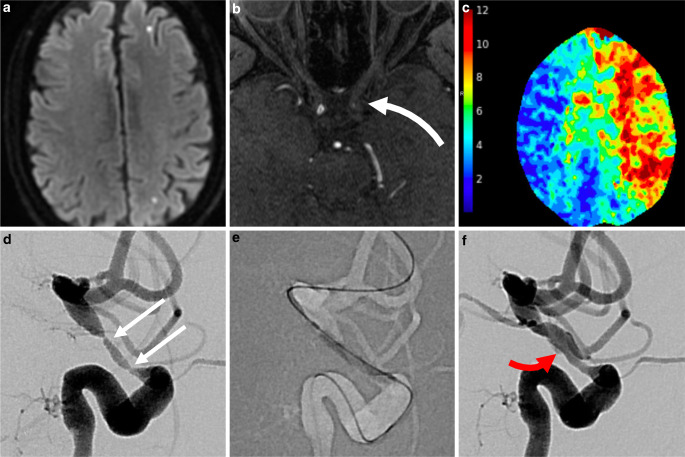
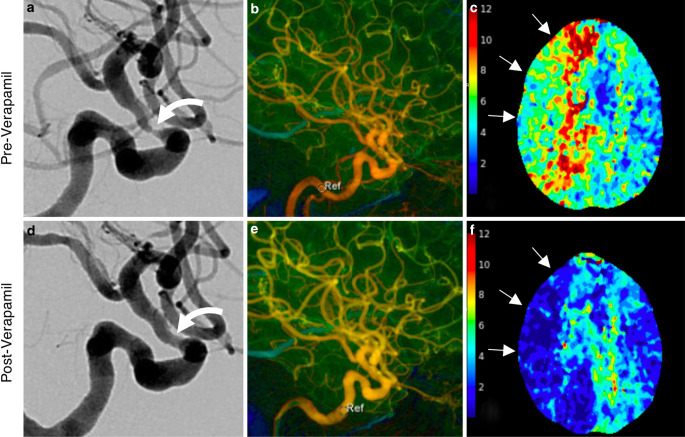
Results: The literature review identified 9 reports of 19 treatments, including percutaneous transluminal angioplasty (PTA) with or without stenting, in 14 patients (mean age 69.6 ± 6.3 years). Out of 12 patients 8 (66.7%) with sufficient data had > 1 pre-existing cardiovascular risk factor. All patients had infarction on MRI while on glucocorticoids and 7/14 (50%) progressed despite adjuvant immunosuppressive agents. Treatment was PTA alone in 15/19 (78.9%) cases and PTA + stent in 4/19 (21.1%). Repeat treatments were performed in 4/14 (28.6%) of patients (PTA-only). Non-flow limiting dissection was reported in 2/19 (10.5%) of treatments. The indications, technical details, and results of PTA are discussed in a single illustrative case. We report the novel use of intra-arterial calcium channel blocker infusion (verapamil) as adjuvant to PTA and as monotherapy, resulting in immediate improvement in cerebral blood flow.
Conclusion: Endovascular treatment, including PTA with or without stenting or calcium channel blocker infusion, may be effective therapies in medically refractory GCA with intracranial stenosis.
Keywords: Angioplasty; Cerebral ischemia; Intracranial stenosis; Vasculitis; Verapamil.
© 2022. The Author(s).
Conflict of interest statement
M. T. Caton Jr., I. T. Mark, K. H. Narsinh, A. Baker, D. L. Cooke, S. W. Hetts, C. F. Dowd, V. V. Halbach, R. T. Higashida, N. U. Ko, S. A. Chung and M. R. Amans declare that they have no competing interests. Amans (unrelated): Board membership: Mind Rhythm; Consultancy: Stryker Neurovascular, Covidien, MicroVention, Comments: Pipeline proctor for Covidien and PHIL DSMB for MicroVention; Patents (planned, pending or issued): Cerebral venous sinus stent, Comments: provisional patent serial number 62/984,549. Dowd (unrelated): Chief Adjudicator for EVOLVE Flow Diverter trial. Department salary support Stryker.
Figures
References
-
- Gonzalez-Gay MA, Vazquez-Rodriguez TR, Gomez-Acebo I, Pego-Reigosa R, Lopez-Diaz MJ, Vazquez-Triñanes MC, Miranda-Filloy JA, Blanco R, Dierssen T, Gonzalez-Juanatey C, Llorca J. Strokes at time of disease diagnosis in a series of 287 patients with biopsy-proven giant cell arteritis. Medicine. 2009;88:227–235. doi: 10.1097/MD.0b013e3181af4518. - DOI - PubMed
-
- Salvarani C, Bella CD, Cimino L, Macchioni P, Formisano D, Bajocchi G, Pipitone N, Catanoso MG, Restuccia G, Ghinoi A, Boiardi L. Risk factors for severe cranial ischaemic events in an Italian population-based cohort of patients with giant cell arteritis. Baillieres Clin Rheumatol. 2009;48:250–253. - PubMed
