

Characterizing the temporal changes in association between modifiable risk factors and acute kidney injury with multi-view analysis
- PMID: 35504130
- PMCID: PMC12516820
- DOI: 10.1016/j.ijmedinf.2022.104785
Characterizing the temporal changes in association between modifiable risk factors and acute kidney injury with multi-view analysis
Abstract
Background: Acute kidney injury (AKI) is a common life-threatening clinical syndrome in hospitalized patients. Advances in machine learning has demonstrated success in AKI risk prediction using electronic health records (EHRs). However, to prevent AKI, it is critical to identify clinically modifiable factors and understand their impact at different prevention windows.
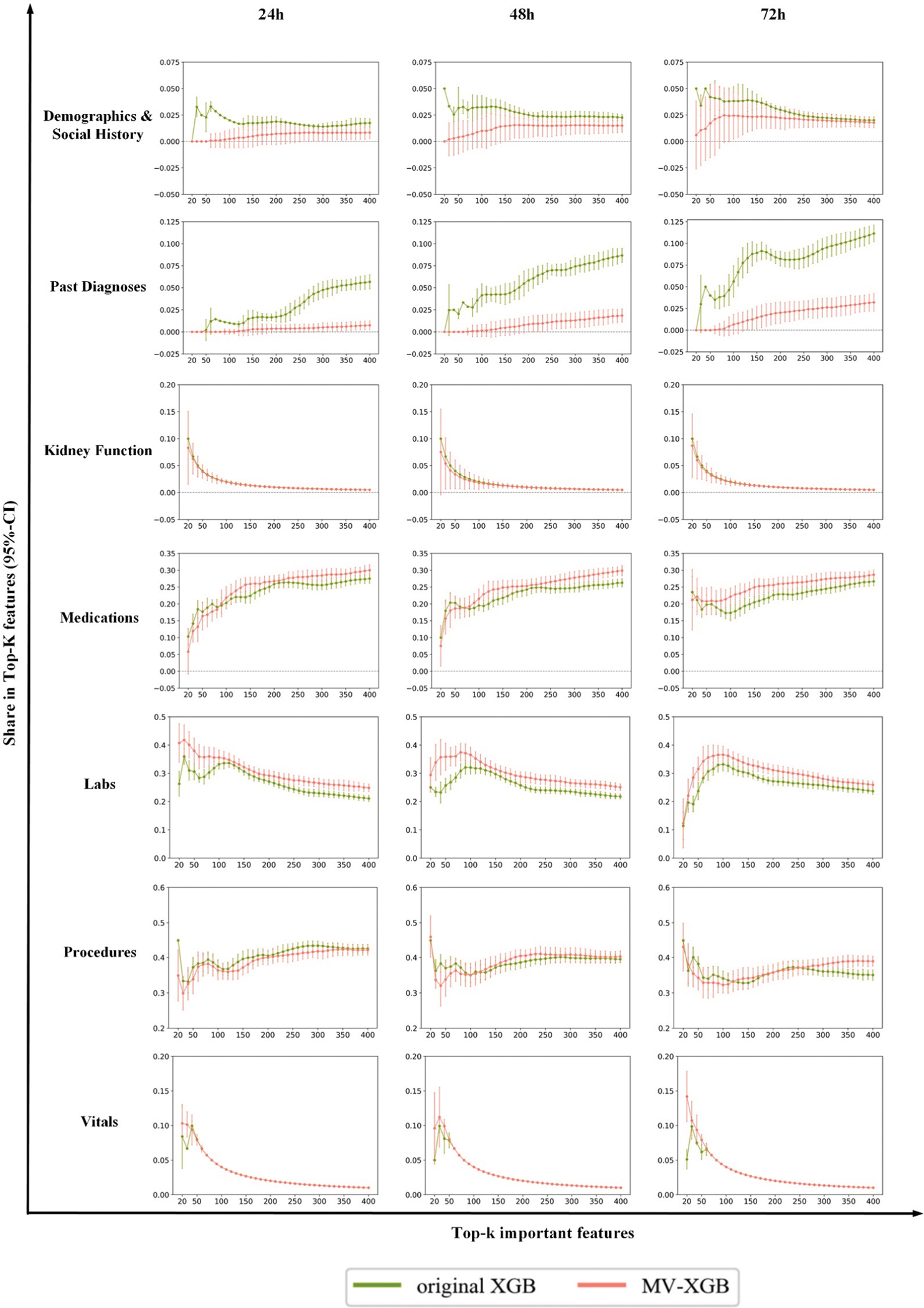
Method: We extracted 4129 clinical variables including demographics, social history, past diagnoses, procedures, labs, medications, vitals from EHRs for a cohort of 144,084 eligible inpatient encounters. We developed a multi-view learning framework for XGBoost (MV-XGB) to enhance algorithm attention on modifiable factors. To study effects of modifiable factors at different time points, we built AKI prediction models at 24-hours, 48-hours, 72-hours before AKI onset. To characterize the temporal changes in effect of modifiable factors on AKI, we derived two indicators, inter-class score-difference and exposed-score-difference, based on SHAP values to compare effects of modifiable factors in different windows.
Result: MV-XGB effectively increased attention on modifiable factors (explained 92.4%-94.1% inter-class score-difference, i.e., predictive difference between AKI and non-AKI samples) while maintaining good predictive performance (AUROCs were 0.854, 0.798, 0.765 in models for 24-48-72 h AKI prediction respectively). We observed that 62% of predicted odds-ratio difference between AKI and non-AKI patients in 24 h can be explained by factors occurring between 24 and 72 h. Among the important modifiable factors, electrolyte balance explained 38.3% of the inter-class score difference increase between 24 h and 72 h, followed by high-risk medications (13.7%), care strategy (12.1%), blood pressure (10%), infection (7.8%), and anemia (5.4%). Effects of cardiac surgery or condition, respiratory ventilation, and anemia remained important longer than 72 h.
Conclusion: Better understanding of the clinically modifiable factors is important to AKI prevention. The proposed multi-view learning approach improved the identification of modifiable factors of AKI and allowed characterization of the temporal dynamics of their potential benefit in intervention.
Keywords: Acute kidney injury; Electronic health records; Machine learning; Multi-view analysis; Prevention.
Copyright © 2022 The Author(s). Published by Elsevier B.V. All rights reserved.
Figures




References
-
- Khwaja A, KDIGO clinical practice guidelines for acute kidney injury, Nephron Clinical, Practice 120 (2012) c179–c184. - PubMed
-
- Chawla LS, Bellomo R, Bihorac A, Goldstein SL, Siew ED, Bagshaw SM, Bittleman D, Cruz D, Endre Z, Fitzgerald RL, Forni L, Kane-Gill SL, Hoste E, Koyner J, Liu KD, Macedo E, Mehta R, Murray P, Nadim M, Ostermann M, Palevsky PM, Pannu N, Rosner M, Wald R, Zarbock A, Ronco C, Kellum JA, Acute kidney disease and renal recovery: consensus report of the Acute Disease Quality Initiative (ADQI) 16 Workgroup, Nat. Rev. Nephrol. 13 (4) (2017) 241–257. - PubMed
-
- Stewart J FG, Smith N, et al. , Adding Insult to Injury: A review of the care of patients who died in hospital with a primary diagnosis of acute kidney injury (acute renal failure), National Confidential Enquiry into Patient Outcome and Death: London, UK, (2009).
-
- Kellum JA, Prowle JR, Paradigms of acute kidney injury in the intensive care setting, Nat. Rev. Nephrol. 14 (4) (2018) 217–230. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
