

Thoracic kyphosis in light of lumbosacral alignment in thoracic adolescent idiopathic scoliosis: recognition of thoracic hypokyphosis and therapeutic implications
- PMID: 35505303
- PMCID: PMC9063219
- DOI: 10.1186/s12891-022-05379-6
Thoracic kyphosis in light of lumbosacral alignment in thoracic adolescent idiopathic scoliosis: recognition of thoracic hypokyphosis and therapeutic implications
Abstract
Background: The uniqueness of spinal sagittal alignment in thoracic adolescent idiopathic scoliosis (AIS), for example, the drastically smaller thoracic kyphosis seen in some patients, has been recognized but not yet fully understood. The purpose of this study was to clarify the characteristics of sagittal alignment of thoracic AIS and to determine the contributing factors.
Methods: Whole spine radiographs of 83 thoracic AIS patients (73 females) were analyzed. The measured radiographic parameters were the Cobb angle of thoracic scoliosis, thoracic kyphosis (TK), lumbar lordosis (LL), C7 sagittal vertical axis (C7 SVA), pelvic incidence (PI), pelvic tilt (PT), and sacral slope (SS). Additionally, max-LL, which was defined as the maximum lordosis angle from the S1 endplate, the inflection point between thoracic kyphosis and lumbar lordosis, and the SVA of the inflection point (IP SVA) were measured. The factors significantly related to a decrease in TK were assessed by stepwise logistic regression analysis. In addition, cluster analysis was performed to classify the global sagittal alignment.
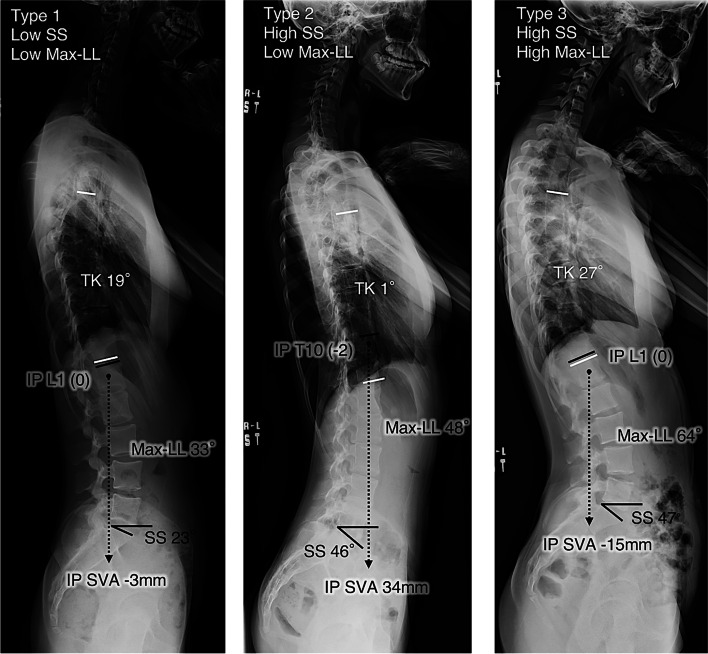
Results: The significant factors for a decrease in TK were an increase in SS (p = 0.0003, [OR]: 1.16) and a decrease in max-LL (p = 0.0005, [OR]: 0.89). According to the cluster analysis, the global sagittal alignment was categorized into the following three types: Type 1 (low SS, low max-LL, n = 28); Type 2 (high SS, low max-LL, n = 22); and Type 3 (high SS, high max-LL, n = 33).
Conclusions: In thoracic AIS, a decreased TK corresponded to an increased SS or a decreased max-LL. The sagittal alignment of thoracic AIS patients could be classified into three types based on SS and max-LL. One of these three types includes the unique sagittal profile of very small TK.
Keywords: Hypokyphosis; Inflection point; Max-LL; Sacral slope; Sagittal alignment; Thoracic AIS.
© 2022. The Author(s).
Figures



Similar articles
-
Sagittal alignment of the cervical spine in the setting of adolescent idiopathic scoliosis.J Neurosurg Spine. 2018 Nov 1;29(5):506-514. doi: 10.3171/2018.3.SPINE171263. Epub 2018 Aug 24. J Neurosurg Spine. 2018. PMID: 30141764
-
Pre- and post-operative sagittal balance in idiopathic scoliosis: a comparison over the ages of two cohorts of 132 adolescents and 52 adults.Eur Spine J. 2013 Mar;22 Suppl 2(Suppl 2):S203-15. doi: 10.1007/s00586-012-2571-x. Epub 2012 Nov 28. Eur Spine J. 2013. PMID: 23188161 Free PMC article.
-
Postoperative changes in sagittal spinopelvic alignment in sitting position in adolescents with idiopathic thoracic scoliosis treated with posterior fusion: an initial analysis.J Neurosurg Pediatr. 2018 Jul;22(1):74-80. doi: 10.3171/2018.2.PEDS17687. Epub 2018 May 4. J Neurosurg Pediatr. 2018. PMID: 29726791
-
Preoperative Sagittal Spinal Profile of Adolescent Idiopathic Scoliosis Lenke Types and Non-Scoliotic Adolescents: A Systematic Review and Meta-Analysis.Spine (Phila Pa 1976). 2019 Jan 15;44(2):134-142. doi: 10.1097/BRS.0000000000002748. Spine (Phila Pa 1976). 2019. PMID: 29927859
-
Analysis of the cervical spine sagittal alignment in young idiopathic scoliosis: a morphological classification of 120 cases.Eur Spine J. 2013 Nov;22(11):2372-81. doi: 10.1007/s00586-013-2753-1. Epub 2013 Apr 12. Eur Spine J. 2013. PMID: 23580056 Free PMC article. Review.
Cited by
-
Patient-Specific Surgical Correction of Adolescent Idiopathic Scoliosis: A Systematic Review.Children (Basel). 2024 Jan 15;11(1):106. doi: 10.3390/children11010106. Children (Basel). 2024. PMID: 38255419 Free PMC article. Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
