

VDI pacing with temporary esophageal and transvenous pacemaker leads to treat post-cardiac surgery cardiogenic shock
- PMID: 35505369
- PMCID: PMC9066848
- DOI: 10.1186/s13019-022-01849-z
VDI pacing with temporary esophageal and transvenous pacemaker leads to treat post-cardiac surgery cardiogenic shock
Abstract
Background: Post-operative atrio-ventricular (AV) block after cardiac surgery is not uncommon in high-risk patients.
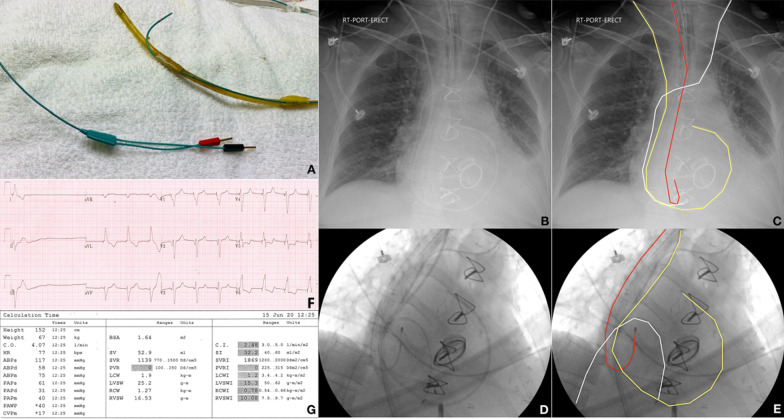
Case presentation: Our case highlights the management of a 62-year-old female with cardiogenic shock post-cardiac surgery with concomitant complete heart block. With VVI pacing proving ineffective, it was postulated that the patient may benefit hemodynamically from AV sequential pacing, re-establishing her atrial kick. We describe a novel technique of attaching a temporary pacemaker wire to an orogastric tube to sense atrial p-waves and pace the ventricle transvenously to perform AV sequential pacing. This was done temporarily to stabilize the patient's hemodynamic status while awaiting a permanent pacemaker implantation.
Conclusions: In hemodynamically unstable post-cardiac surgery patients with complete heart block in whom VVI pacing fails to improve their clinical status, clinicians should consider VDI pacing with an orogastric atrial sensing pacemaker lead, in consultation with the cardiac surgeon and the electrophysiology team. Of note, the patient needs to have underlying organized atrial activity for this setup to work.
Keywords: Cardiogenic shock; Case report; Heart block; Pacing; Post-cardiac surgery.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Pérez Vela JL, Jiménez Rivera JJ, Alcalá Llorente M, González de Marcos B, Torrado H, García Laborda C, et al. Low cardiac output syndrome in the postoperative period of cardiac surgery. Profile, differences in clinical course and prognosis. The ESBAGA study. Med Intensiva. 2018;42(3):159–167. doi: 10.1016/j.medin.2017.05.009. - DOI - PubMed
-
- Anier A, Kaik J, Meigas K. A novel method for reducing pain sensation at transesophageal atrial stimulation. Conf Proc IEEE Eng Med Biol Soc. 2007;2007:923–926. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
