

Evaluation of the Results of Minimally Invasive Plate Osteosynthesis Using a Locking Plate in the Treatment of Distal Femur Fractures
- PMID: 35505714
- PMCID: PMC9053357
- DOI: 10.7759/cureus.23617
Evaluation of the Results of Minimally Invasive Plate Osteosynthesis Using a Locking Plate in the Treatment of Distal Femur Fractures
Abstract
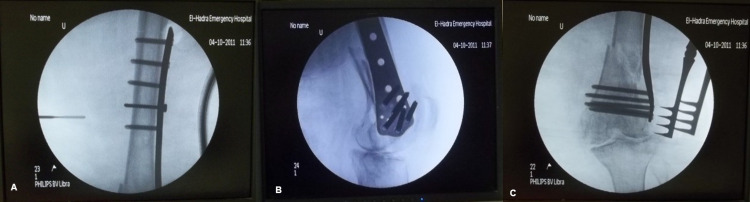
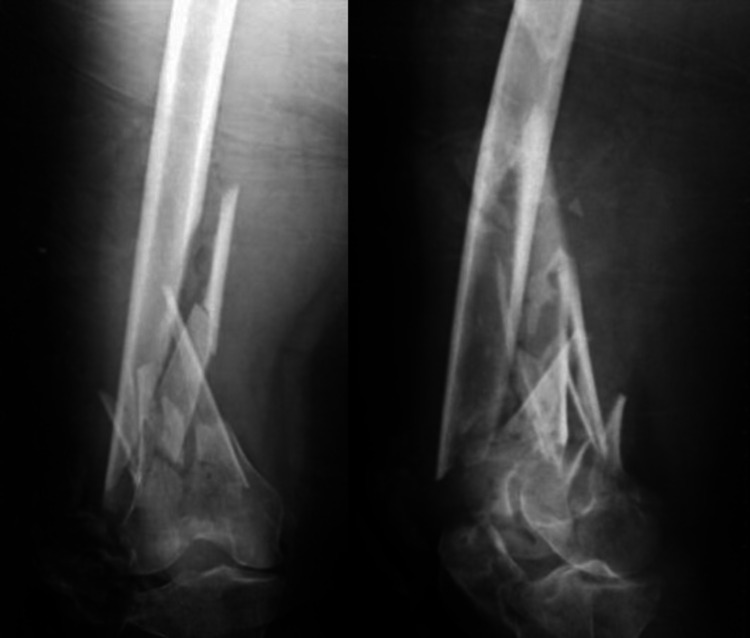
Introduction Distal femur fractures are serious injuries that can be difficult to treat, carry an unpredictable prognosis, and lead to long-term disability and morbidity. The introduction of minimally invasive plate osteosynthesis (MIPO) avoids direct exposure of the fracture site, improves fracture healing and decreases the incidence of complications. The aim of this study was to assess prospectively the early results of the treatment of supracondylar fractures of the femur using minimally invasive percutaneous osteosynthesis using a distal femoral locking plate. The study was a prospective study that included 20 adult patients who sustained distal femur fractures. Materials and methods The study was a prospective study that included 20 patients suffering from supracondylar fractures of the femur. All patients had fixation of the fracture using a distal femur locking plate (less invasive stabilization system (LISS)) in a minimally invasive technique using an anterolateral or direct lateral approach to the distal femur according to the fracture classification. The follow-up was done using the functional evaluation scale for distal femoral fractures as regards range of motion, deformation, pain, walking ability, and return to work. Results The mean age was 52.80 (19-80) years. The mean body mass index of the patients was 28.50, with a range of 23-43 kg/m2. The mechanism of trauma was road traffic accidents (RTAs) in nine patients (45%) and falling from standing height in eleven patients (55%). Fractures were classified according to the Arbeitsgemeinschaft Osteosynthesefragen-Orthopedic Trauma Association (AO-OTA) classification. All patients were followed up for a period of six months and assessed in terms of knee range of motion, deformation, pain, walking ability, and return to work. The mean time of radiological union, in which bony trabeculae crossed the fracture gap, was 3.45 ± 0.79 months. The final results obtained were excellent in four patients (20%), good in nine patients (45%), fair in five patients (25%), and poor in two patients (10%). Complications encountered were knee stiffness (20%), superficial wound infection (10%), and shortening (15%). Conclusion LISS plating using the MIPO approach is useful in treating complex distal femoral fractures. Large studies from independent centers reporting long-term results are needed to further evaluate the role of LISS plating and the MIPO approach in the management of complex distal femoral fractures.
Keywords: distal femur fracture; liss; locking plate; minimally invasive surgery; mipo.
Copyright © 2022, Abdelmonem et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures






Similar articles
-
[Osteosynthesis for periprosthetic supracondylar fracture above a total knee arthroplasty using a locking compression plate].Acta Chir Orthop Traumatol Cech. 2009 Dec;76(6):473-8. Acta Chir Orthop Traumatol Cech. 2009. PMID: 20067694 Czech.
-
The use of interfragmentary positional screw in minimally invasive plate osteosynthesis for simple distal femur fractures in elderly patients: A retrospective, single-centre pilot study.Injury. 2016 Dec;47(12):2795-2799. doi: 10.1016/j.injury.2016.10.034. Epub 2016 Oct 29. Injury. 2016. PMID: 27802890
-
Minimally invasive plate osteosynthesis with dual plating for periprosthetic distal femoral fractures following total knee arthroplasty.J Orthop Surg Res. 2021 Jul 6;16(1):433. doi: 10.1186/s13018-021-02586-0. J Orthop Surg Res. 2021. PMID: 34229703 Free PMC article.
-
Non-union in lateral locked plating for distal femoral fractures: A systematic review.Injury. 2019 Nov;50(11):1790-1794. doi: 10.1016/j.injury.2019.07.012. Epub 2019 Jul 13. Injury. 2019. PMID: 31324342
-
Dual-Plating in Distal Femur Fracture: A Systematic Review and Limited Meta-analysis.Indian J Orthop. 2021 Aug 23;56(2):183-207. doi: 10.1007/s43465-021-00489-0. eCollection 2022 Feb. Indian J Orthop. 2021. PMID: 35140850 Free PMC article. Review.
Cited by
-
Using a Traction Table for Fracture Reduction during Minimally Invasive Plate Osteosynthesis (MIPO) of Distal Femoral Fractures Provides Anatomical Alignment.J Clin Med. 2023 Jun 14;12(12):4044. doi: 10.3390/jcm12124044. J Clin Med. 2023. PMID: 37373737 Free PMC article.
References
-
- Epidemiology of adult fractures: a review. Court-Brown CM, Caesar B. Injury. 2006;37:691–697. - PubMed
-
- The epidemiology of fractures of the distal femur. Martinet O, Cordey J, Harder Y, Maier A, Bühler M, Barraud GE. Injury. 2000;31:62–63. - PubMed
-
- Evolution of minimally invasive plate osteosynthesis (MIPO) in the femur. Krettek C, Müller M, Miclau T. Injury. 2001;32:14–23. - PubMed
-
- Less invasive stabilisation system plating for distal femoral fractures. Kanabar P, Kumar V, Owen PJ, Rushton N. J Orthop Surg. 2007;15:299–302. - PubMed
-
- Transarticular approach and retrograde plate osteosynthesis (TARPO): an alternative surgical approach for complex distal intra-articular femur fractures. Krettek C, Miclau T, Stephan C, Tscheme H. Tech Orthop. 1999;14:219–229.
LinkOut - more resources
Full Text Sources
Miscellaneous