

Magnetic resonance imaging of musculoskeletal infections
- PMID: 35505859
- PMCID: PMC9047866
- DOI: 10.5114/pjr.2022.113825
Magnetic resonance imaging of musculoskeletal infections
Abstract
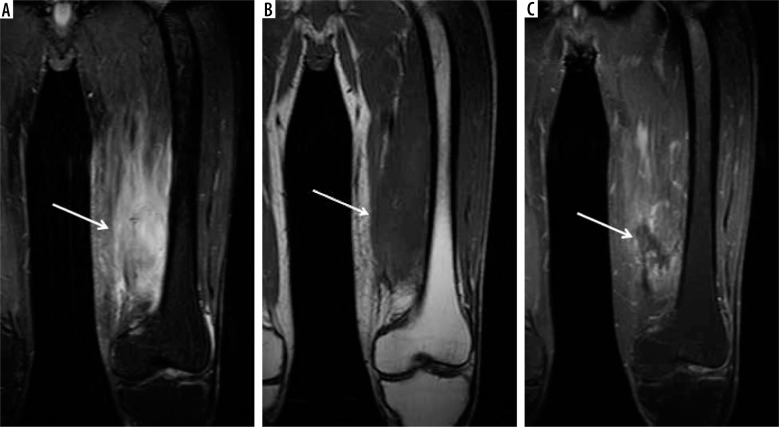
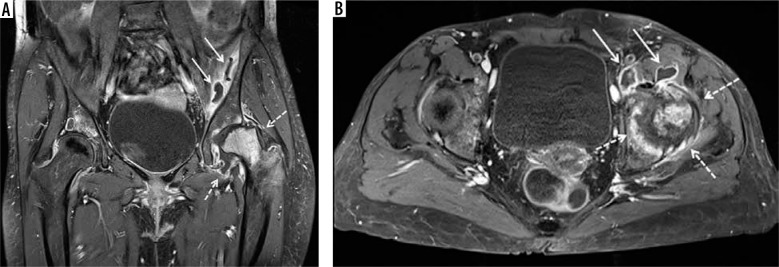
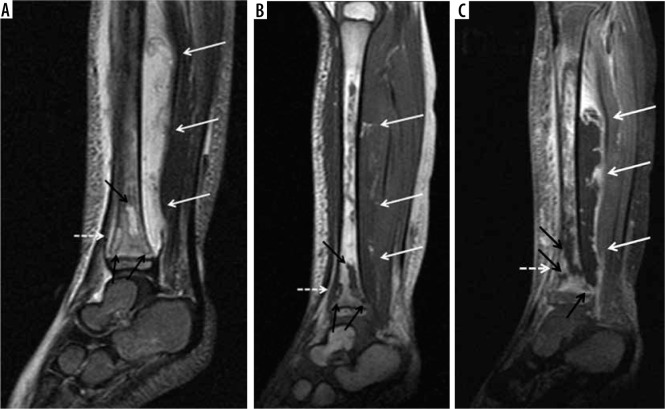
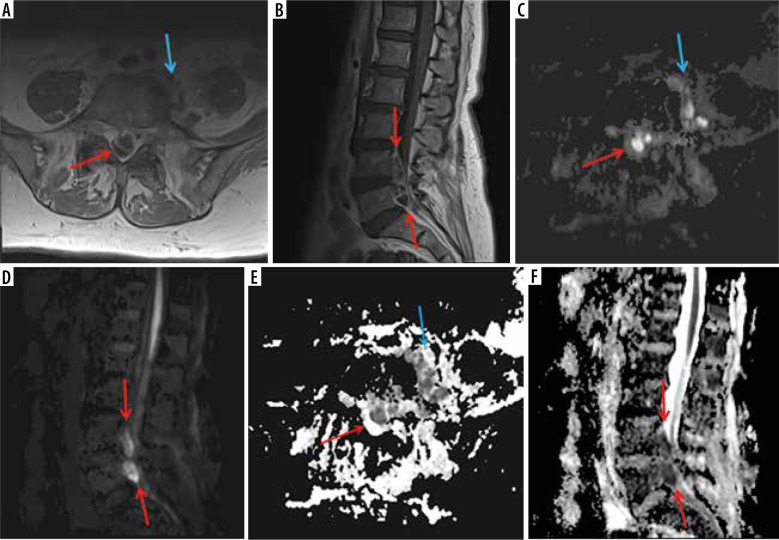
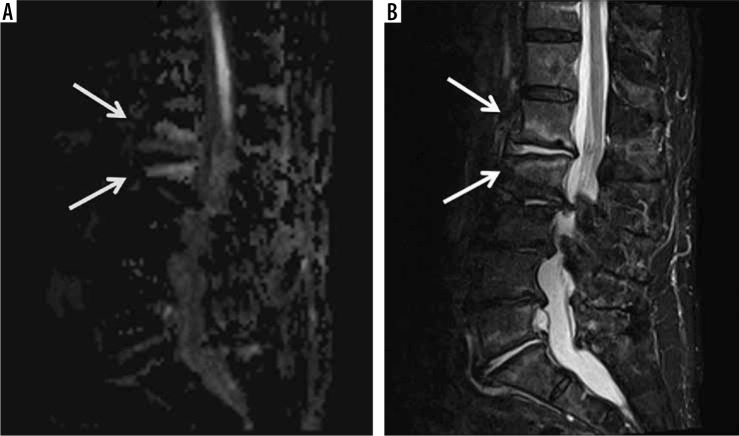
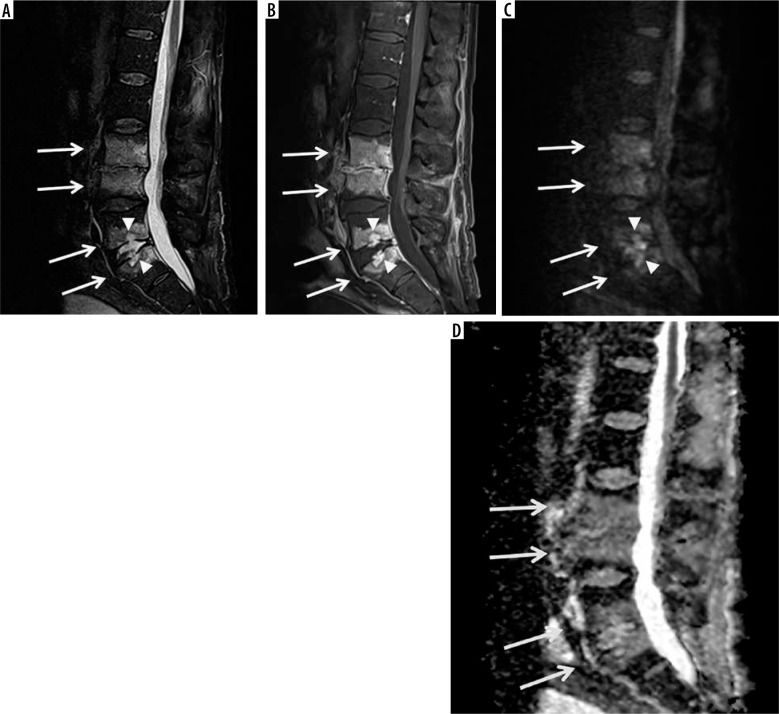
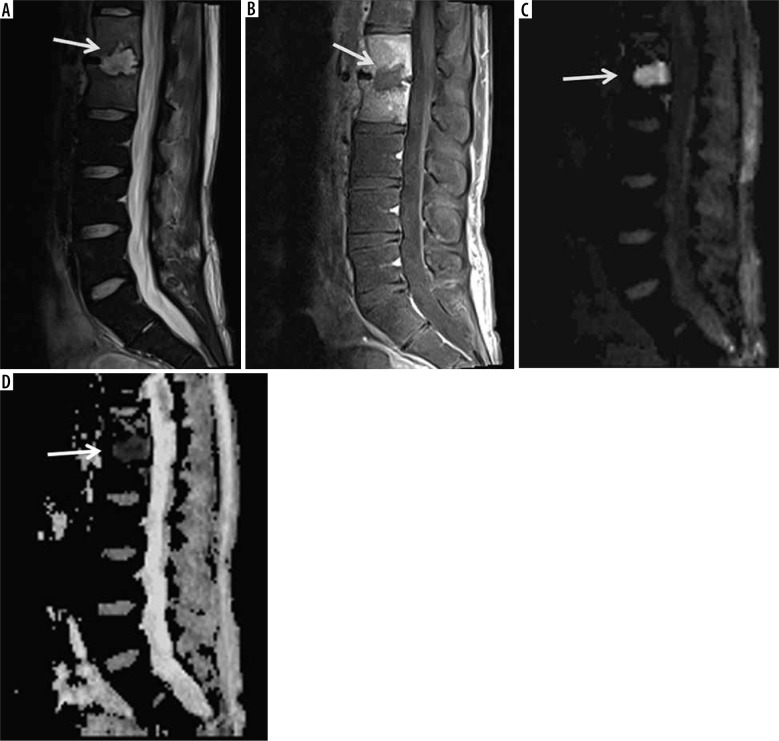
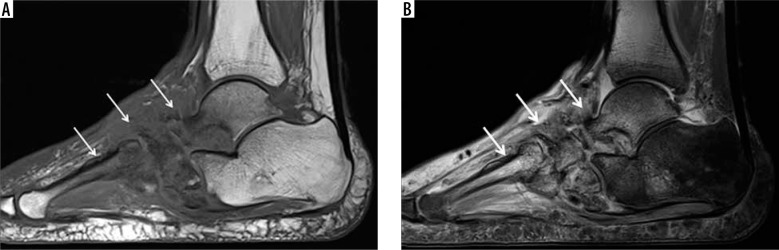
Magnetic resonance imaging (MRI) is a powerful imaging modality in the evaluation of musculoskeletal (MSK) soft tissue, joint, and bone infections. It allows prompt diagnosis and assessment of the extent of disease, which permits timely treatment to optimize long-term clinical outcomes. MRI is highly sensitive and specific in detecting the common findings of MSK infections, such as superficial and deep soft tissue oedema, joint, bursal and tendon sheath effusions, lymphadenopathy, bone marrow oedema, erosive bone changes and periostitis, and bone and cartilage destruction and sequestration. Contrast-enhanced MRI allows detection of non-enhancing fluid collections and necrotic tissues, rim-enhancing abscesses, heterogeneously or diffusely enhancing phlegmons, and enhancing active synovitis. Diffusion-weighted imaging (DWI) is useful in detecting soft-tissue abscesses, particularly in patients who cannot receive gadolinium-based intravenous contrast. MRI is less sensitive than computed tomography (CT) in detecting soft-tissue gas. This article describes the pathophysiology of pyogenic MSK infections, including the route of contamination and common causative organisms, typical MR imaging findings of various soft tissue infections including cellulitis, superficial and deep fasciitis and necrotizing fasciitis, pyomyositis, infectious bursitis, infectious tenosynovitis, and infectious lymphadenitis, and of joint and bone infections including septic arthritis and osteomyelitis (acute, subacute, and chronic). The authors also discuss MRI findings and pitfalls related to infected hardware and diabetic foot infections, and briefly review standards of treatment of various pyogenic MSK infections.
Keywords: MRI; cellulitis; fasciitis; osteomyelitis; pyomyositis; septic arthritis.
© Pol J Radiol 2022.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures








References
-
- Turecki MB, Taljanovic MS, Stubbs AY, et al. . Imaging of musculoskeletal soft tissue infections. Skeletal Radiol 2010; 39: 957-971. - PubMed
-
- Headley AJ. Necrotizing soft tissue infections: a primary care review. Am Fam Physician 2003; 68: 323-328. - PubMed
-
- Hill MK, Sanders CV. Skin and soft tissue infections in critical care. Crit Care Clin 1998; 14: 251-262. - PubMed
-
- Expert Panel on Musculoskeletal Imaging; Beaman FD, von Herrmann PF, Kransdorf MJ, et al. . ACR Appropriateness Criteria(®) suspected osteomyelitis, septic arthritis, or soft tissue infection (excluding spine and diabetic foot). J Am Coll Radiol 2017; 14 (5S): S326-S337. - PubMed
-
- Walker EA, Beaman FD, Wessell DE, et al. . ACR Appropriateness Criteria® suspected osteomyelitis of the foot in patients with diabetes mellitus. J Am Coll Radiol 2019, 16 (11S): S440-S450. - PubMed
Publication types
LinkOut - more resources
Full Text Sources