

A multi-institutional prospective observational study to evaluate fascia iliaca compartment block (FICB) for preventing delirium in adults with hip fracture
- PMID: 35505910
- PMCID: PMC9014076
- DOI: 10.1136/tsaco-2022-000904
A multi-institutional prospective observational study to evaluate fascia iliaca compartment block (FICB) for preventing delirium in adults with hip fracture
Abstract
Objectives: Until recently, systemic opioids have been standard care for acute pain management of geriatric hip fracture; however, opioids increase risk for delirium. Fascia Iliaca compartment blocks (FICB) may be favored to systemic analgesia for reducing delirium, but this has not been well demonstrated. We evaluated the efficacy of adjunctive FICB versus systemic analgesia on delirium incidence, opioid consumption, and pain scores.
Methods: This prospective, observational cohort study was performed in patients (55-90 years) with traumatic hip fracture admitted to five trauma centers within 12 hours of injury, enrolled between January 2019 and November 2020. The primary end point was development of delirium, defined by the Confusion Assessment Method tool, from arrival through 48 hours postoperatively, and analyzed with multivariate Firth logistic regression. Secondary end points were analyzed with analysis of covariance models and included preoperative and postoperative oral morphine equivalents and pain numeric rating scale scores.
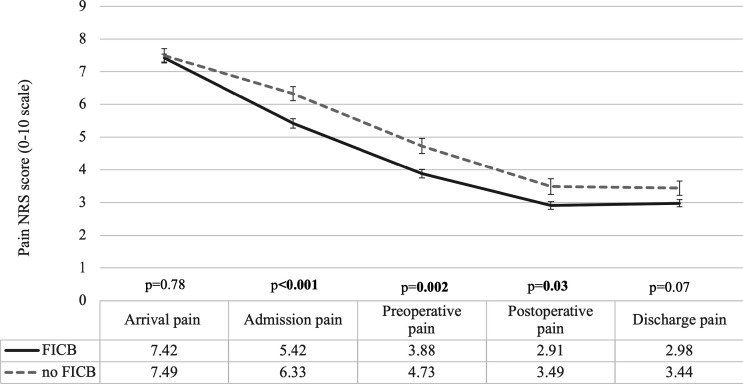
Results: There were 517 patients enrolled, 381 (74%) received FICB and 136 (26%) did not. Delirium incidence was 5.4% (n=28) and was similar for patients receiving FICB versus no FICB (FICB, 5.8% and no FICB, 4.4%; adjusted OR: 1.2 (95% CI 0.5 to 3.0), p=0.65). Opioid requirements were similar for patients receiving FICB and no FICB, preoperatively (p=0.75) and postoperatively (p=0.51). Pain scores were significantly lower with FICB than no FICB, preoperatively (4.2 vs 5.1, p=0.002) and postoperatively (2.9 vs 3.5, p=0.04).
Conclusions: FICB demonstrated significant benefit on self-reported pain but without a concomitant reduction in opioid consumption. Regarding delirium incidence, these findings suggest clinical equipoise and the need for a randomized trial.
Level of evidence: II-prospective, therapeutic.
Keywords: analgesics, opioid; geriatrics; hip fractures; nerve blocks.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Does time to surgery for traumatic hip fracture impact the efficacy of fascia iliaca blocks? A brief report.Trauma Surg Acute Care Open. 2022 Nov 15;7(1):e000970. doi: 10.1136/tsaco-2022-000970. eCollection 2022. Trauma Surg Acute Care Open. 2022. PMID: 36407296 Free PMC article.
-
The Analgesic effect of adding ultrasound-guided pericapsular nerve group block to suprainguinal fascia iliaca compartment block for hip fracture surgery: A prospective randomized controlled trial.Medicine (Baltimore). 2023 Nov 3;102(44):e35649. doi: 10.1097/MD.0000000000035649. Medicine (Baltimore). 2023. PMID: 37932971 Free PMC article. Clinical Trial.
-
Fascia Iliaca Block in Hip and Femur Fractures to Reduce Opioid Use.J Emerg Med. 2022 Jul;63(1):1-9. doi: 10.1016/j.jemermed.2022.04.018. Epub 2022 Aug 4. J Emerg Med. 2022. PMID: 35933265
-
The Application of Fascia Iliaca Compartment Block for Acute Pain Control of Hip Fracture and Surgery.Curr Pain Headache Rep. 2021 Mar 11;25(4):22. doi: 10.1007/s11916-021-00940-9. Curr Pain Headache Rep. 2021. PMID: 33694008 Review.
-
Ultrasound-Guided Suprainguinal Fascia Iliaca Compartment Block in Patients Undergoing Hip Surgery: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.Cureus. 2024 Sep 25;16(9):e70147. doi: 10.7759/cureus.70147. eCollection 2024 Sep. Cureus. 2024. PMID: 39463554 Free PMC article. Review.
Cited by
-
Pain relief for femur fractures using Fascia Iliaca Block and IV fentanyl.Bioinformation. 2025 Mar 31;21(3):567-570. doi: 10.6026/973206300210567. eCollection 2025. Bioinformation. 2025. PMID: 40599913 Free PMC article.
-
Does time to surgery for traumatic hip fracture impact the efficacy of fascia iliaca blocks? A brief report.Trauma Surg Acute Care Open. 2022 Nov 15;7(1):e000970. doi: 10.1136/tsaco-2022-000970. eCollection 2022. Trauma Surg Acute Care Open. 2022. PMID: 36407296 Free PMC article.
-
Comparative efficacy of fascia iliaca compartment block using liposomal bupivacaine versus ropivacaine for preoperative analgesia in elderly patients with intertrochanteric femur fracture: a randomised controlled trial protocol.BMJ Open. 2025 Jul 16;15(7):e093756. doi: 10.1136/bmjopen-2024-093756. BMJ Open. 2025. PMID: 40669908 Free PMC article.
-
Understanding the association between pain and delirium in older hospital inpatients: systematic review and meta-analysis.Age Ageing. 2024 Apr 1;53(4):afae073. doi: 10.1093/ageing/afae073. Age Ageing. 2024. PMID: 38610062 Free PMC article.
-
Comparison of traditional systemic analgesic, single shot or continuous fascia iliaca compartment block for pain management in patients with hip or proximal femoral fractures: A protocol for systematic review and network meta-analysis.PLoS One. 2025 Mar 26;20(3):e0319988. doi: 10.1371/journal.pone.0319988. eCollection 2025. PLoS One. 2025. PMID: 40138268 Free PMC article.
References
-
- National Center for Health Statistics . Trends in health and aging. Hyatsville, MD: US Department of Health and Human Services, 2006.
LinkOut - more resources
Full Text Sources
Research Materials