

Trends in 10-Year Outcomes Among Medicare Beneficiaries Who Survived an Acute Myocardial Infarction
- PMID: 35507330
- PMCID: PMC9069341
- DOI: 10.1001/jamacardio.2022.0662
Trends in 10-Year Outcomes Among Medicare Beneficiaries Who Survived an Acute Myocardial Infarction
Abstract
Importance: Short-term outcomes after acute myocardial infarction (AMI) have improved, but little is known about longer-term outcomes.
Objective: To evaluate trends in 10-year all-cause mortality and hospitalization for recurrent AMI by demographic subgroups and examine the association between recurrence and mortality.
Design, setting, and participants: Medicare fee-for-service beneficiaries who survived after AMI from 1995 to 2019. Subgroups were defined by age, sex, race, dual Medicare-Medicaid-eligible status, and residence in health priority areas (geographic areas with persistently high adjusted mortality and hospitalization rates). Data were analyzed from October 2020 to February 2022.
Exposure: Medicare fee-for-service beneficiaries who survived an AMI.
Main outcomes and measures: Ten-year all-cause mortality and hospitalization for recurrent AMI, beginning 30 days from the index AMI admission.
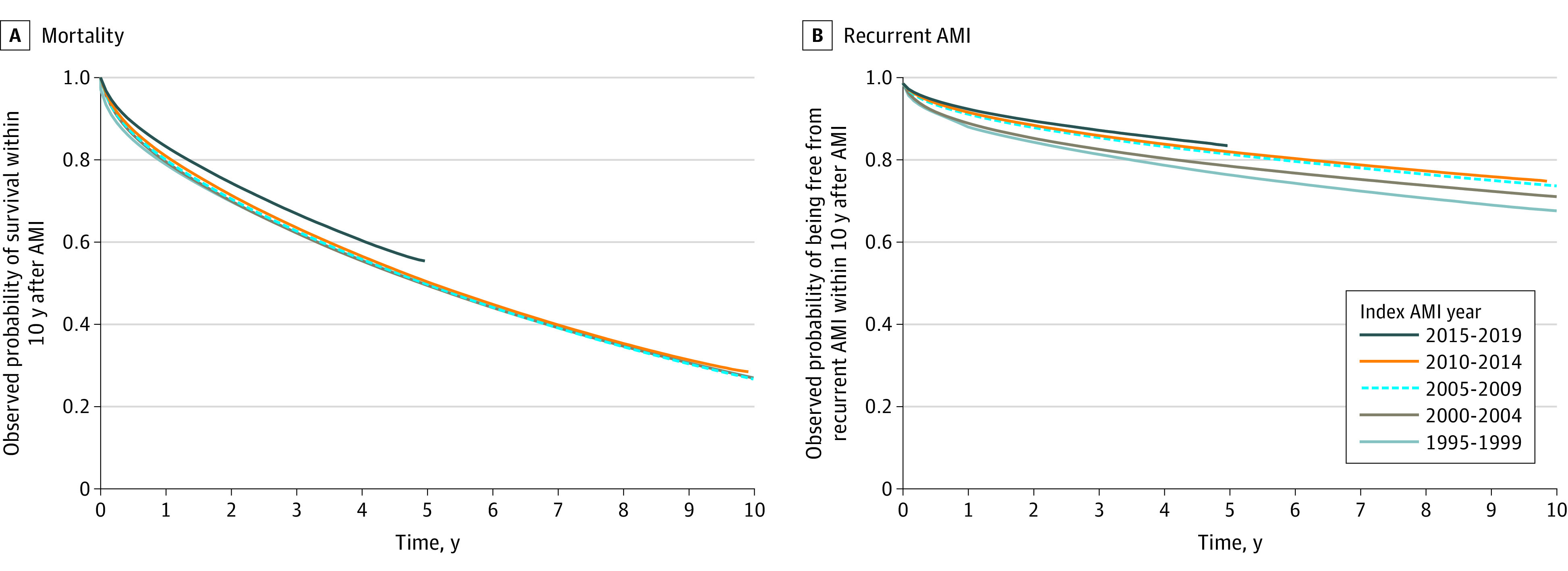
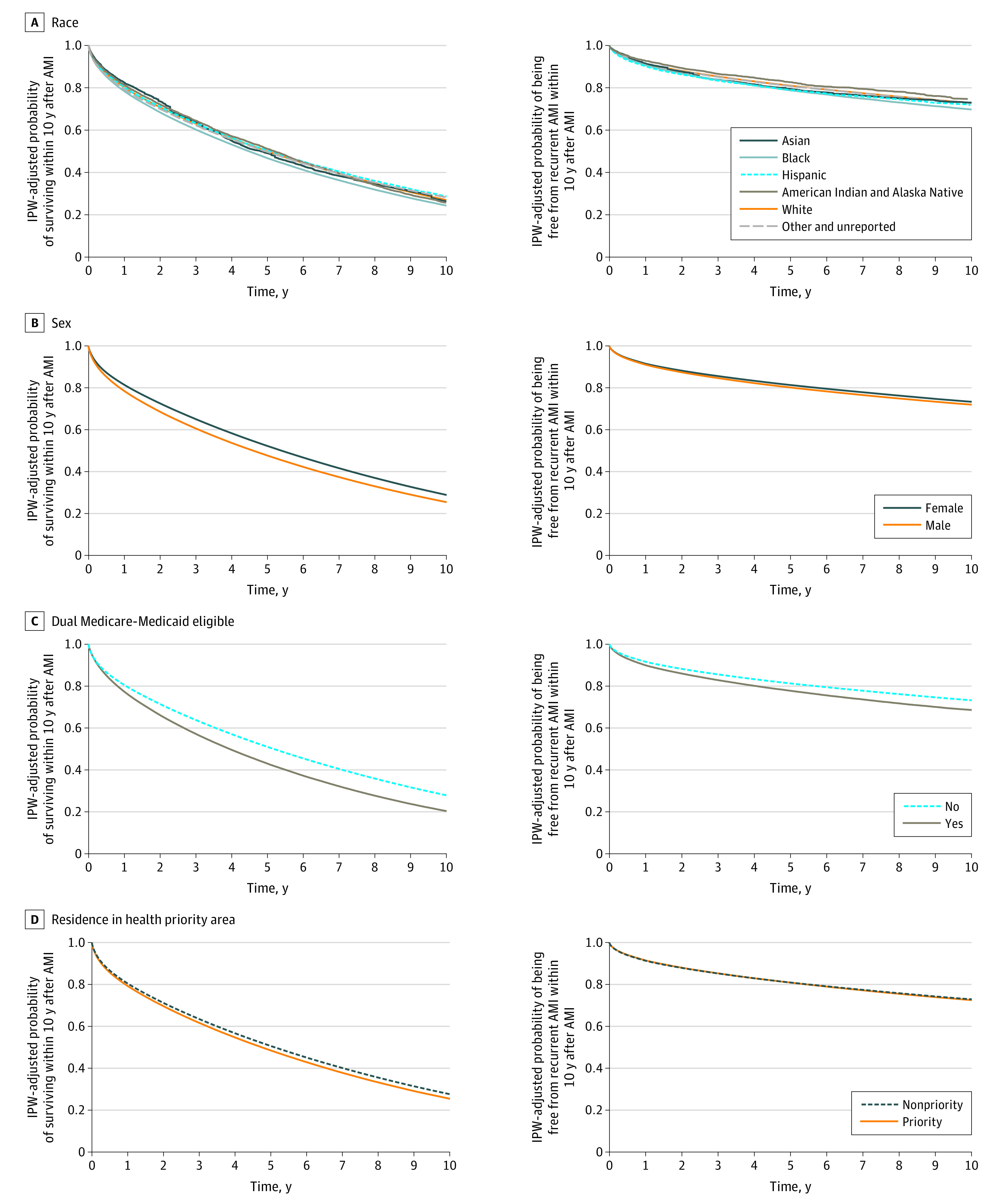
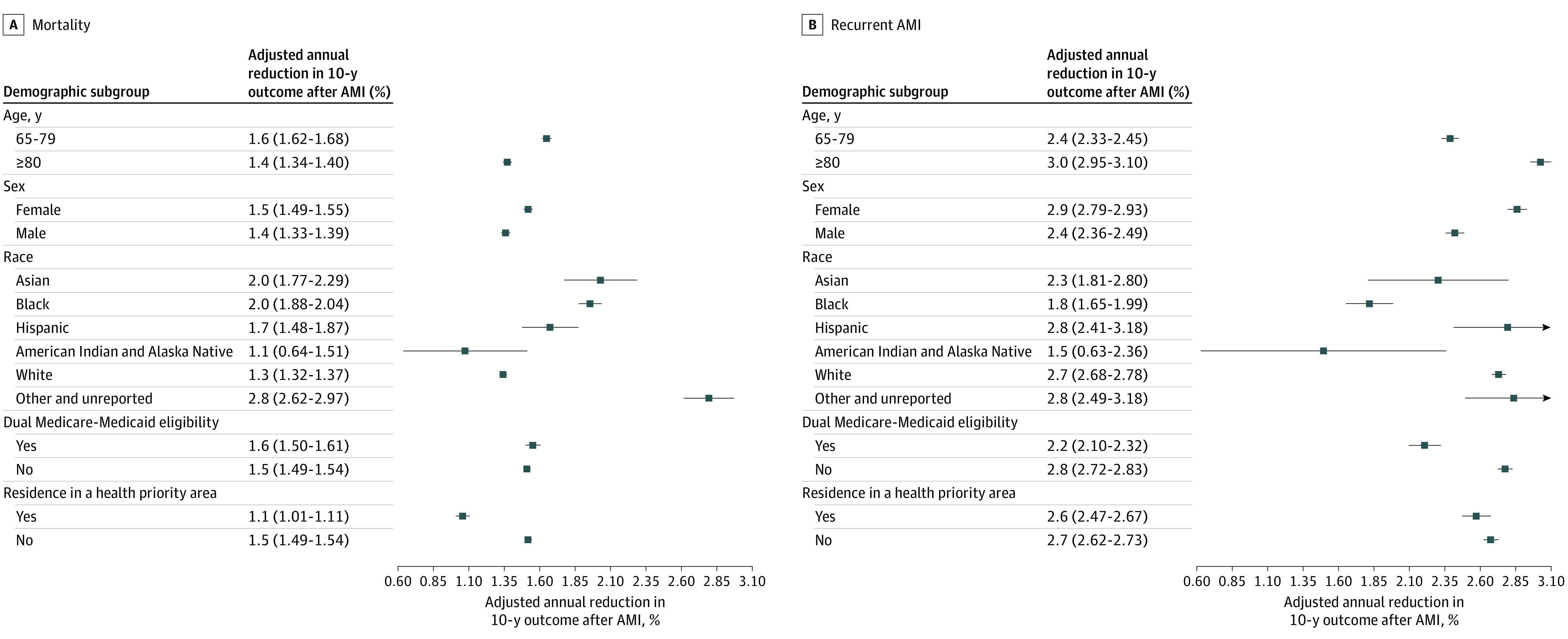
Results: Of an included 3 982 266 AMI survivors, 1 952 450 (49.0%) were female, and the mean (SD) age was 78.0 (7.4) years. Ten-year mortality and recurrent AMI rates were 72.7% (95% CI, 72.6-72.7) and 27.1% (95% CI, 27.0-27.2), respectively. Adjusted annual reductions were 1.5% (95% CI, 1.4-1.5) for mortality and 2.7% (95% CI, 2.6-2.7) for recurrence. In subgroup analyses balancing patient characteristics, hazard ratios (HRs) for mortality and recurrence were 1.13 (95% CI, 1.12-1.13) and 1.07 (95% CI, 1.06-1.07), respectively, for men vs women; 1.05 (95% CI, 1.05-1.06) and 1.08 (95% CI, 1.07-1.09) for Black vs White patients; 0.96 (95% CI, 0.95-0.96) and 1.00 (95% CI, 1.00-1.01) for other race (including American Indian and Alaska Native, Asian, Hispanic, other race or ethnicity, and unreported) vs White patients; 1.24 (95% CI, 1.24-1.24) and 1.21 (95% CI, 1.20-1.21) for dual Medicare-Medicaid-eligible vs non-dual Medicare-Medicaid-eligible patients; and 1.06 (95% CI, 1.06-1.07) and 1.00 (95% CI, 1.00-1.01) for patients in health priority areas vs other areas. For patients hospitalized in 2007 to 2009, the last 3 years for which full 10-year follow-up data were available, 10-year mortality risk was 13.9% lower than for those hospitalized in 1995 to 1997 (adjusted HR, 0.86; 95% CI, 0.85-0.87) and 10-year recurrence risk was 22.5% lower (adjusted HR, 0.77; 95% CI, 0.76-0.78). Mortality within 10 years after the initial AMI was higher for patients with a recurrent AMI (80.6%; 95% CI, 80.5-80.7) vs those without recurrence (72.4%; 95% CI, 72.3-72.5).
Conclusions and relevance: In this study, 10-year mortality and hospitalization for recurrence rates improved over the last decades for patients who survived the acute period of AMI. There were marked differences in outcomes and temporal trends across demographic subgroups, emphasizing the urgent need for prioritization of efforts to reduce inequities in long-term outcomes.
Conflict of interest statement
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
