

Stereotactic body radiotherapy versus surgery for early-stage non-small cell lung cancer: an updated meta-analysis involving 29,511 patients included in comparative studies
- PMID: 35508065
- PMCID: PMC9064643
- DOI: 10.36416/1806-3756/e20210390
Stereotactic body radiotherapy versus surgery for early-stage non-small cell lung cancer: an updated meta-analysis involving 29,511 patients included in comparative studies
Abstract
Objective: To evaluate the efficacy of stereotactic body radiotherapy (SBRT) versus surgery for early-stage non-small cell lung cancer (NSCLC) by means of a meta-analysis of comparative studies.
Methods: Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses and Meta-analysis of Observational Studies in Epidemiology guidelines, searches were performed on PubMed, MEDLINE, Embase, and Cochrane Library for eligible studies. The meta-analysis compared the hazard ratios (HR) for overall survival (OS), cancer-specific survival (CSS), and local control (LC). Subgroup and meta-regression analyses evaluated the association of extent of surgical resection, study publication year, tumor staging, propensity score matching, proportion of chemotherapy use, and proportion of pathological lymph node involvement with CSS and OS.
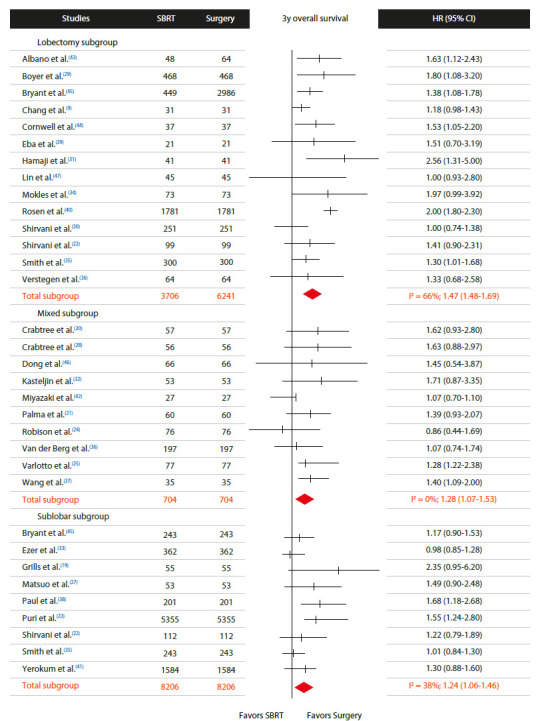
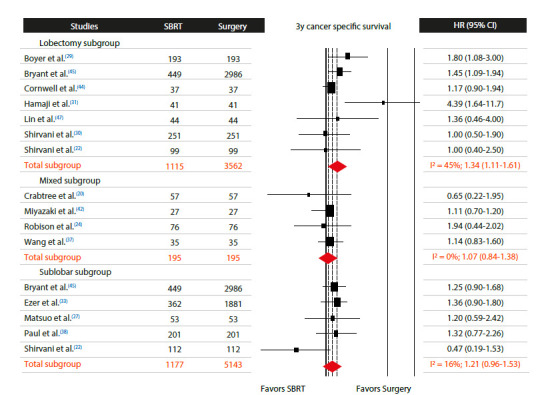
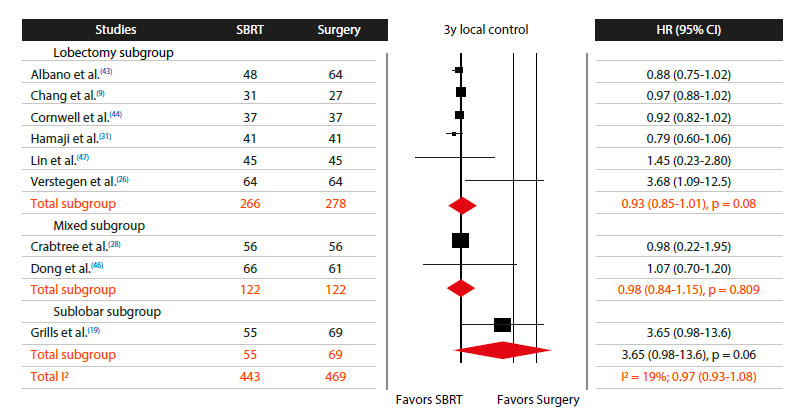
Results: Thirty studies involving 29,511 patients were included (surgery group: 17,146 patients and SBRT group: 12,365 patients). There was a significant difference in favor of surgery vs. SBRT in the 3-year OS (HR = 1.35; 95% CI: 1.22-1.44; I2 = 66%) and 3-year CSS (HR = 1.23; 95% CI: 1.09-1.37; I2 = 17%), but not in the 3-year LC (HR = 0.97; 95% CI: 0.93-1.08; I2 = 19%). In the subgroup analysis for OS, no significant difference between surgery and SBRT groups was observed in the T1N0M0 subgroup (HR = 1.26; 95% CI: 0.95-1.68; I2 = 0%). In subgroup analysis for CSS, no significant difference was detected between the sublobar resection subgroup and the SBRT group (HR = 1.21; 95% CI: 0.96-1.53; I2 = 16%).
Conclusions: Surgery generally resulted in better 3-year OS and CSS than did SBRT; however, publication bias and heterogeneity may have influenced these findings. In contrast, SBRT produced LC results similar to those of surgery regardless of the extent of surgical resection. These findings may have important clinical implications for patients with comorbidities, advanced age, poor pulmonary reserve, and other factors that may contraindicate surgery.
Objetivo:: Avaliar a eficácia da stereotactic body radiotherapy (SBRT, radioterapia estereotáxica corporal) vs. cirurgia para câncer de pulmão de células não pequenas em estágio inicial por meio de uma meta-análise de estudos comparativos.
Métodos:: Seguindo as diretrizes Preferred Reporting Items for Systematic Reviews and Meta-Analyses e Meta-analysis of Observational Studies in Epidemiology, foram realizadas buscas no PubMed, MEDLINE, Embase e Cochrane Library por estudos elegíveis. A meta-análise comparou as razões de risco (RR) para sobrevida global (SG), sobrevida específica para câncer (SEC) e controle local (CL). As análises de subgrupo e metarregressão avaliaram a associação de extensão da ressecção cirúrgica, ano de publicação do estudo, estadiamento do tumor, correspondência de escore de propensão, porcentagem de quimioterapia e porcentagem de acometimento linfonodal com SEC e SG.
Resultados:: Trinta estudos envolvendo 29.511 pacientes foram incluídos (grupo cirurgia: 17.146 pacientes e grupo SBRT: 12.365 pacientes). Houve diferença significativa a favor da cirurgia vs. SBRT na SG em 3 anos (RR = 1,35; IC95%: 1,22-1,44; I2 = 66%) e na SEC em 3 anos (RR = 1,23; IC95%: 1,09-1,37; I2 = 17%), mas não no CL em 3 anos (RR = 0,97; IC95%: 0,93-1,08; I2 = 19%). Na análise de subgrupo para SG, nenhuma diferença significativa entre os grupos cirurgia e SBRT foi observada no subgrupo T1N0M0 (RR = 1,26; IC95%: 0,95-1,68; I2 = 0%). Na análise de subgrupo para SEC, nenhuma diferença significativa foi detectada entre o subgrupo ressecção sublobar e o grupo SBRT (RR = 1,21; IC95%: 0,96-1,53; I2 = 16%).
Conclusões:: A cirurgia geralmente resultou em melhor SG e SEC em 3 anos do que a SBRT; no entanto, viés de publicação e heterogeneidade podem ter influenciado esses achados. Já a SBRT produziu resultados de CL semelhantes aos da cirurgia, independentemente da extensão da ressecção cirúrgica. Esses achados podem ter implicações clínicas importantes para pacientes com comorbidades, idade avançada, baixa reserva pulmonar e outros fatores que possam contraindicar a cirurgia.
Conflict of interest statement
Figures
References
-
- Govindan R, Page N, Morgensztern D, Read W, Tierney R, Vlahiotis A. Changing epidemiology of small-cell lung cancer in the United States over the last 30 years analysis of the surveillance, epidemiologic, and end results database. J Clin Oncol. 2006;24(28):4539–4544. doi: 10.1200/JCO.2005.04.4859. - DOI - PubMed
-
- Fernandez FG, Kosinski AS, Burfeind W, Park B, DeCamp MM, Seder C. The Society of Thoracic Surgeons Lung Cancer Resection Risk Model Higher Quality Data and Superior Outcomes [published correction appears in Ann Thorac. Surg. 2017;104(2):726–726. doi: 10.1016/j.athoracsur.2016.02.098. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
