

Patient-derived micro-organospheres enable clinical precision oncology
- PMID: 35508177
- PMCID: PMC9177814
- DOI: 10.1016/j.stem.2022.04.006
Patient-derived micro-organospheres enable clinical precision oncology
Abstract
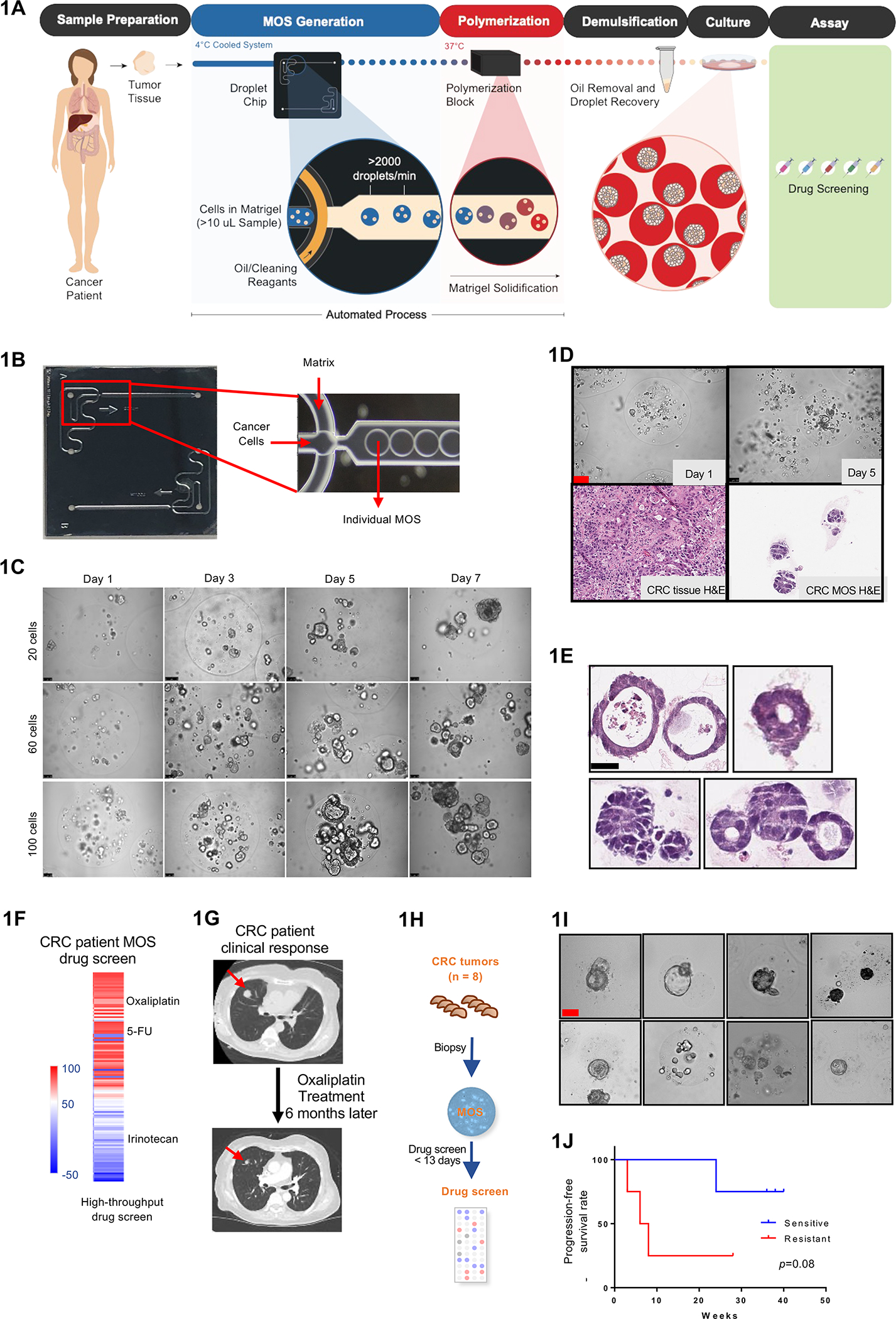
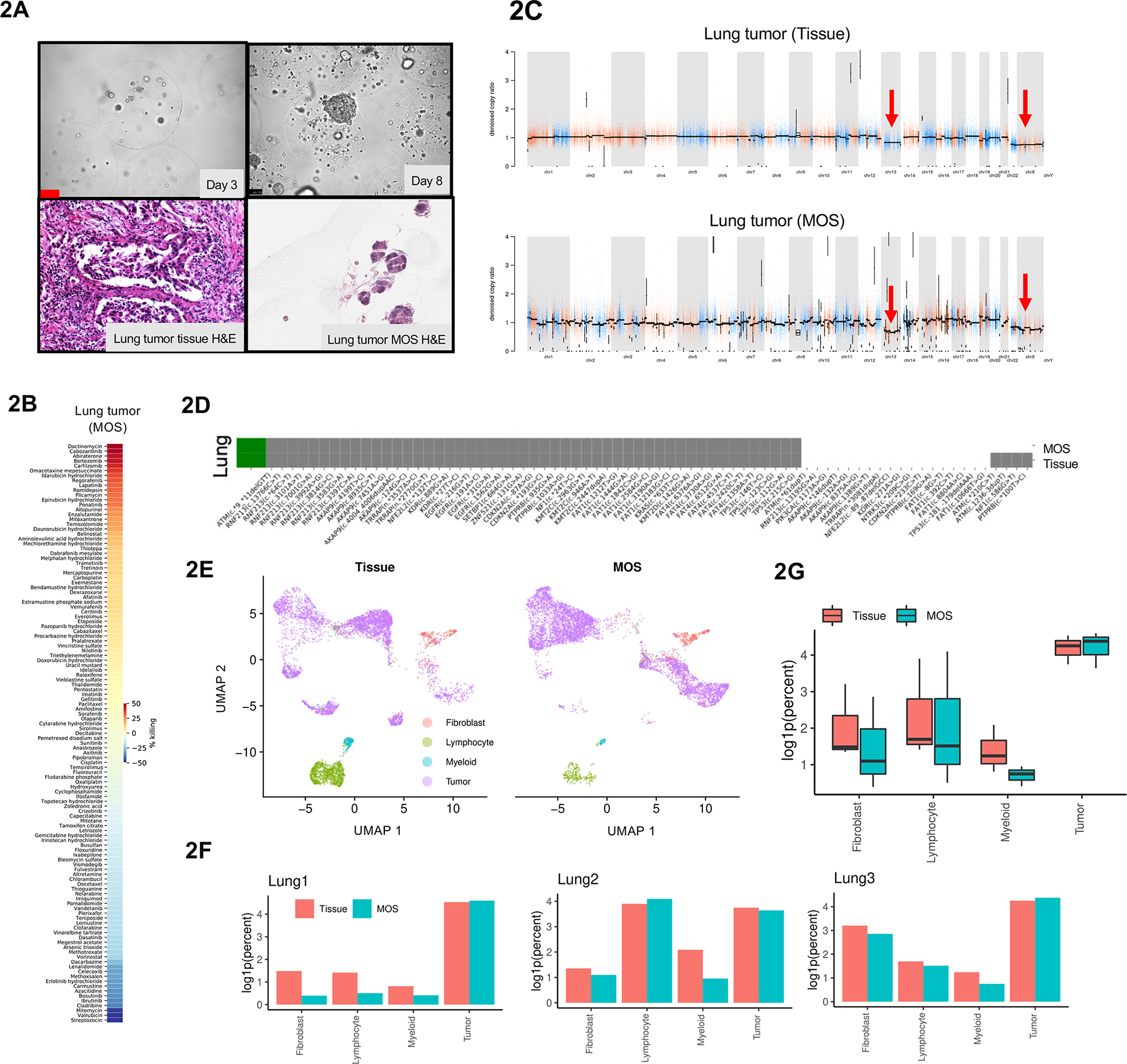
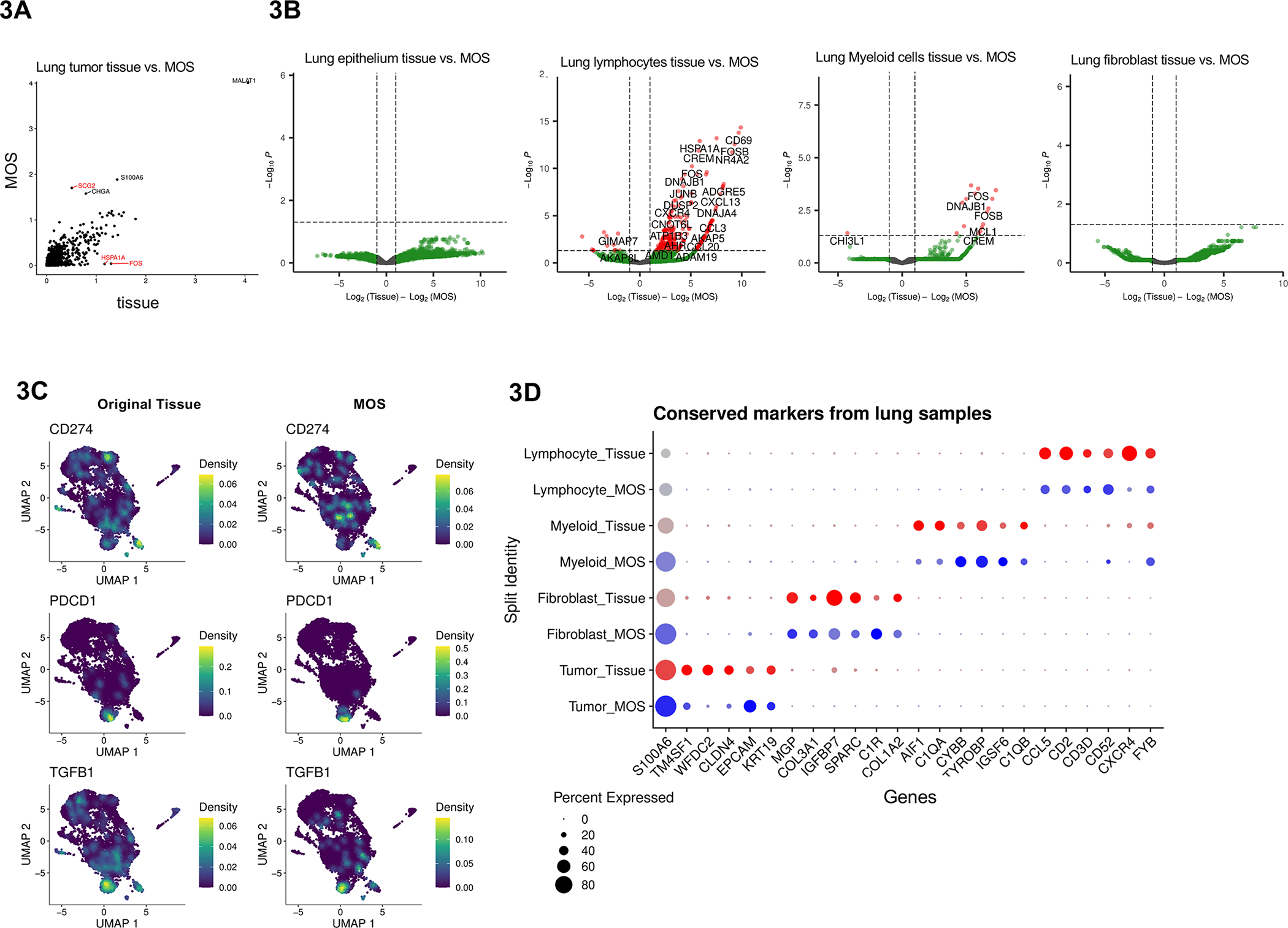
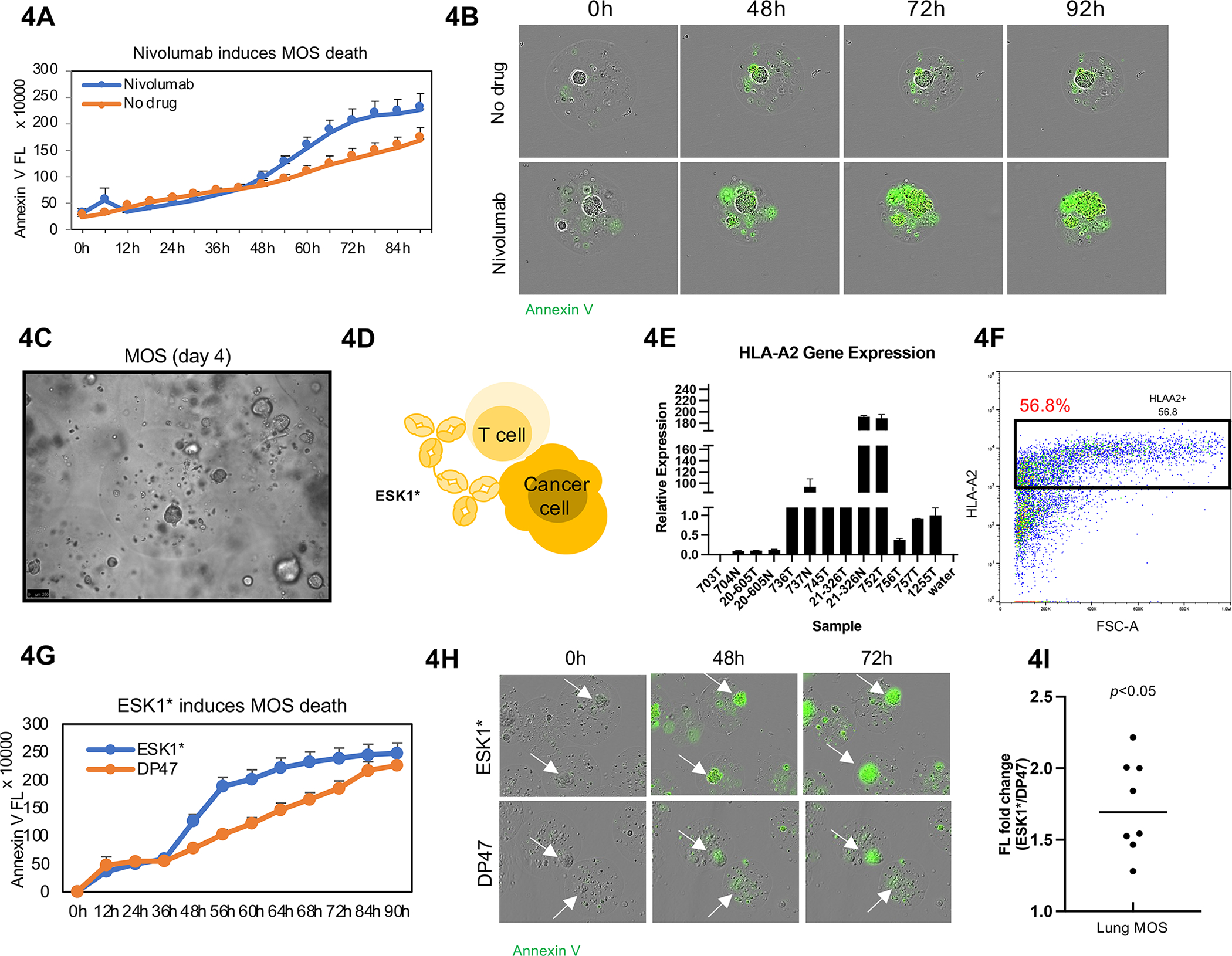
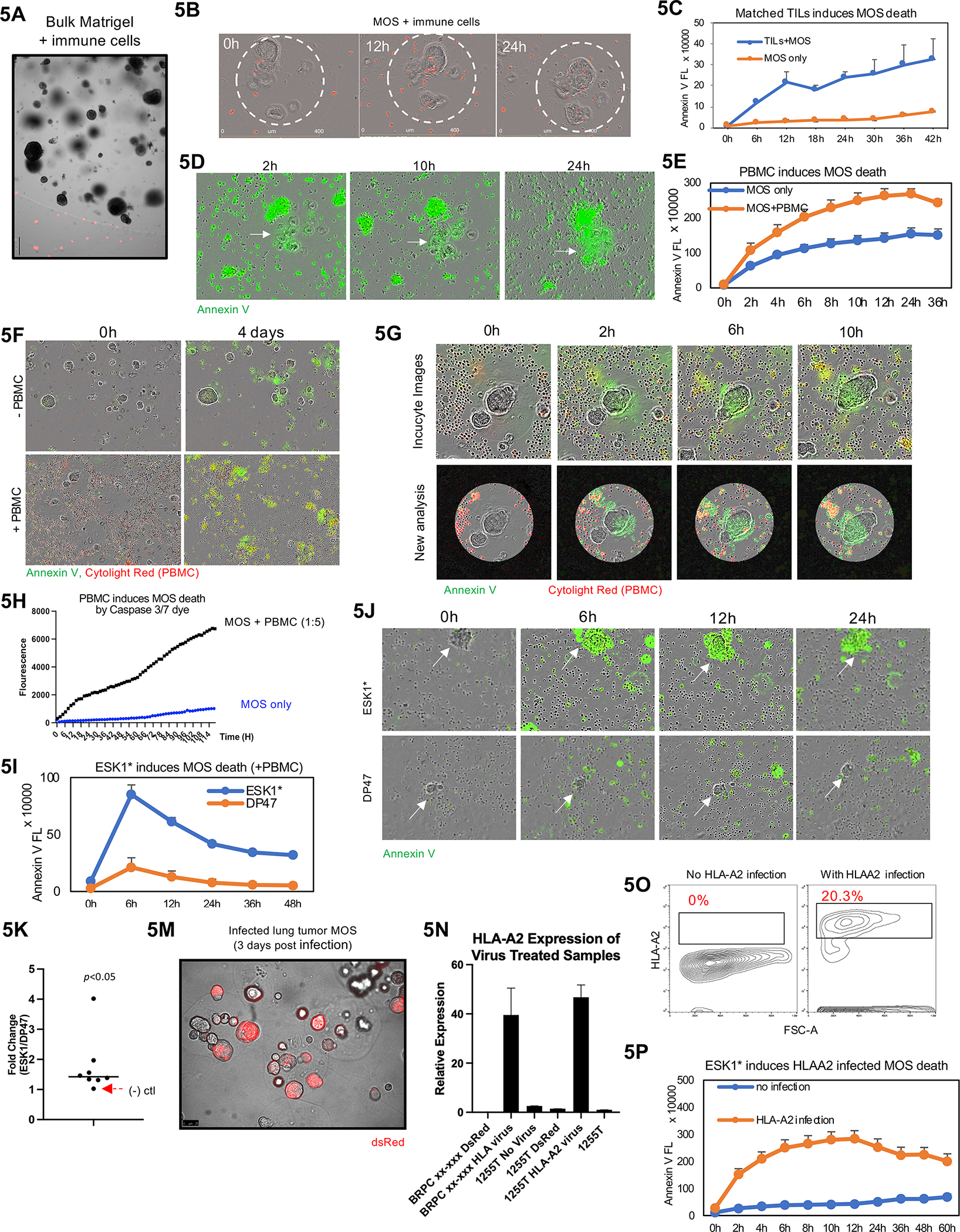
Patient-derived xenografts (PDXs) and patient-derived organoids (PDOs) have been shown to model clinical response to cancer therapy. However, it remains challenging to use these models to guide timely clinical decisions for cancer patients. Here, we used droplet emulsion microfluidics with temperature control and dead-volume minimization to rapidly generate thousands of micro-organospheres (MOSs) from low-volume patient tissues, which serve as an ideal patient-derived model for clinical precision oncology. A clinical study of recently diagnosed metastatic colorectal cancer (CRC) patients using an MOS-based precision oncology pipeline reliably assessed tumor drug response within 14 days, a timeline suitable for guiding treatment decisions in the clinic. Furthermore, MOSs capture original stromal cells and allow T cell penetration, providing a clinical assay for testing immuno-oncology (IO) therapies such as PD-1 blockade, bispecific antibodies, and T cell therapies on patient tumors.
Keywords: adoptive cell therapy; bispecific antibody; colorectal cancer; droplet microfluidics; immune-oncology; lung cancer; micro-organosphere; precision medicine; precision oncology; tumorsphere.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests X.S., D.H., and H.C. are cofounders of Xilis Inc. H.C. is an employee of Roche and on the advisory board of Cell Stem Cell. H.C.’s full disclosure is given at https://www.uu.nl/staff/JCClevers/. S.D. and Z.W. performed the majority of the study at Duke University and now are employees of Xilis Inc. Patents WO2020242594 and US 2021/0285054 are related to this work.
Figures
Comment in
-
Expanding the precision oncology toolkit with micro-organospheres for early cancer diagnosis.Cell Stem Cell. 2022 Jun 2;29(6):873-875. doi: 10.1016/j.stem.2022.05.002. Cell Stem Cell. 2022. PMID: 35659872
Similar articles
-
Rapid tissue prototyping with micro-organospheres.Stem Cell Reports. 2022 Sep 13;17(9):1959-1975. doi: 10.1016/j.stemcr.2022.07.016. Epub 2022 Aug 18. Stem Cell Reports. 2022. PMID: 35985334 Free PMC article.
-
Expanding the precision oncology toolkit with micro-organospheres for early cancer diagnosis.Cell Stem Cell. 2022 Jun 2;29(6):873-875. doi: 10.1016/j.stem.2022.05.002. Cell Stem Cell. 2022. PMID: 35659872
-
Implementing patient derived organoids in functional precision medicine for patients with advanced colorectal cancer.J Exp Clin Cancer Res. 2023 Oct 25;42(1):281. doi: 10.1186/s13046-023-02853-4. J Exp Clin Cancer Res. 2023. PMID: 37880806 Free PMC article.
-
Personalized Immuno-Oncology.Med Princ Pract. 2021;30(1):1-16. doi: 10.1159/000511107. Epub 2020 Aug 25. Med Princ Pract. 2021. PMID: 32841942 Free PMC article. Review.
-
Organoid in colorectal cancer: progress and challenges.Chin Med J (Engl). 2020 Aug 20;133(16):1971-1977. doi: 10.1097/CM9.0000000000000882. Chin Med J (Engl). 2020. PMID: 32826461 Free PMC article. Review.
Cited by
-
Patient-derived organoids (PDOs) and PDO-derived xenografts (PDOXs): New opportunities in establishing faithful pre-clinical cancer models.J Natl Cancer Cent. 2022 Oct 22;2(4):263-276. doi: 10.1016/j.jncc.2022.10.001. eCollection 2022 Dec. J Natl Cancer Cent. 2022. PMID: 39036550 Free PMC article. Review.
-
Activation of Cytotoxic Lymphocytes Through CD6 Enhances Killing of Cancer Cells.Res Sq [Preprint]. 2023 Oct 9:rs.3.rs-3405677. doi: 10.21203/rs.3.rs-3405677/v1. Res Sq. 2023. Update in: Cancer Immunol Immunother. 2024 Jan 27;73(2):34. doi: 10.1007/s00262-023-03578-1. PMID: 37886483 Free PMC article. Updated. Preprint.
-
In vitro 3D modeling of colorectal cancer: the pivotal role of the extracellular matrix, stroma and immune modulation.Front Genet. 2025 May 1;16:1545017. doi: 10.3389/fgene.2025.1545017. eCollection 2025. Front Genet. 2025. PMID: 40376304 Free PMC article. Review.
-
Improved drug-screening tests of candidate anti-cancer drugs in patient-derived xenografts through use of numerous measures of tumor growth determined in multiple independent laboratories.PLoS One. 2025 Jun 18;20(6):e0324141. doi: 10.1371/journal.pone.0324141. eCollection 2025. PLoS One. 2025. PMID: 40531816 Free PMC article.
-
Cancer-on-a-chip for precision cancer medicine.Lab Chip. 2025 Jul 8;25(14):3314-3347. doi: 10.1039/d4lc01043d. Lab Chip. 2025. PMID: 40376718 Free PMC article. Review.
References
-
- (2018). Organoids May Point to Best Therapy. Cancer discovery 8, 524–524. - PubMed
-
- Besser MJ, Shapira-Frommer R, Treves AJ, Zippel D, Itzhaki O, Schallmach E, Kubi A, Shalmon B, Hardan I, Catane R, et al. (2009). Minimally cultured or selected autologous tumor-infiltrating lymphocytes after a lympho-depleting chemotherapy regimen in metastatic melanoma patients. J Immunother 32, 415–423. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
