

Venovenous extracorporeal membrane oxygenation in patients with acute covid-19 associated respiratory failure: comparative effectiveness study
- PMID: 35508314
- PMCID: PMC9065544
- DOI: 10.1136/bmj-2021-068723
Venovenous extracorporeal membrane oxygenation in patients with acute covid-19 associated respiratory failure: comparative effectiveness study
Abstract
Objective: To estimate the effect of extracorporeal membrane oxygenation (ECMO) compared with conventional mechanical ventilation on outcomes of patients with covid-19 associated respiratory failure.
Design: Observational study.
Setting: 30 countries across five continents, 3 January 2020 to 29 August 2021.
Participants: 7345 adults admitted to the intensive care unit with clinically suspected or laboratory confirmed SARS-CoV-2 infection.
Interventions: ECMO in patients with a partial pressure of arterial oxygen to fraction of inspired oxygen (PaO2/FiO2) ratio <80 mm Hg compared with conventional mechanical ventilation without ECMO.
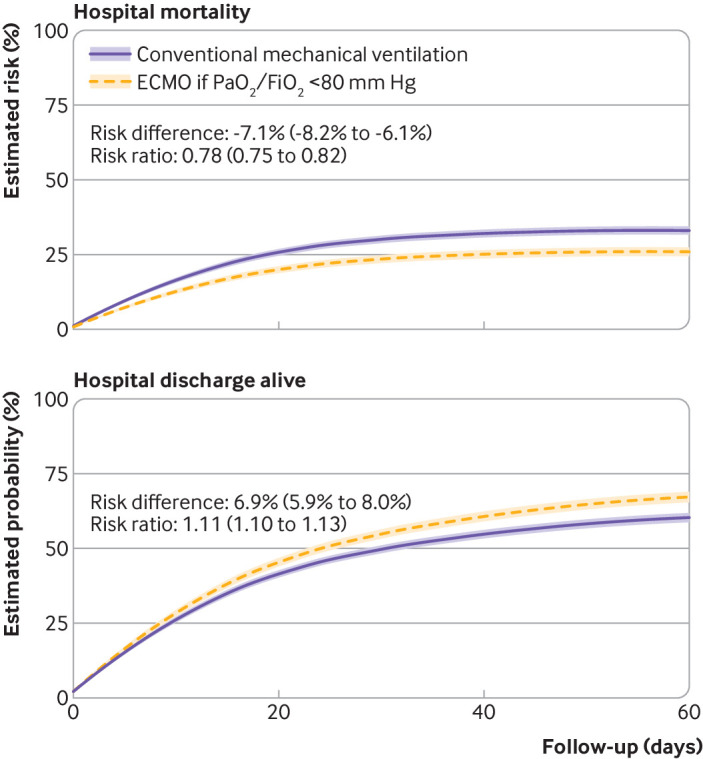
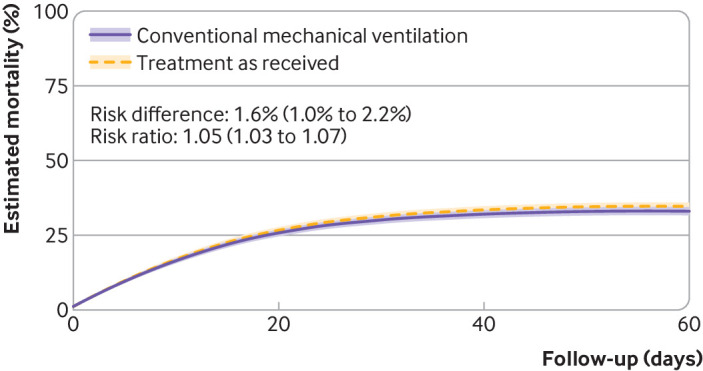
Main outcome measure: The primary outcome was hospital mortality within 60 days of admission to the intensive care unit. Adherence adjusted estimates were calculated using marginal structural models with inverse probability weighting, accounting for competing events and for baseline and time varying confounding.
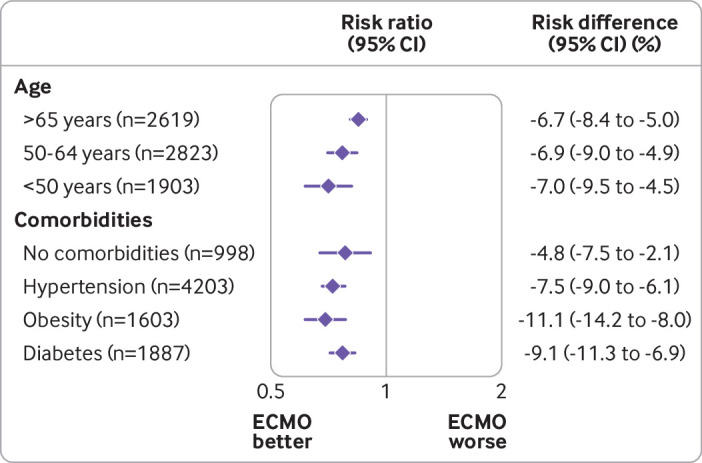
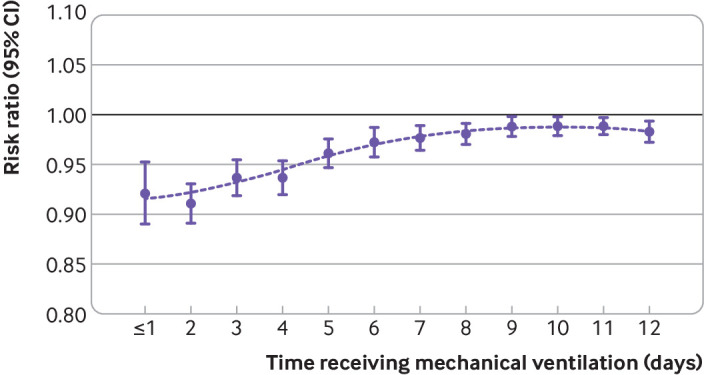
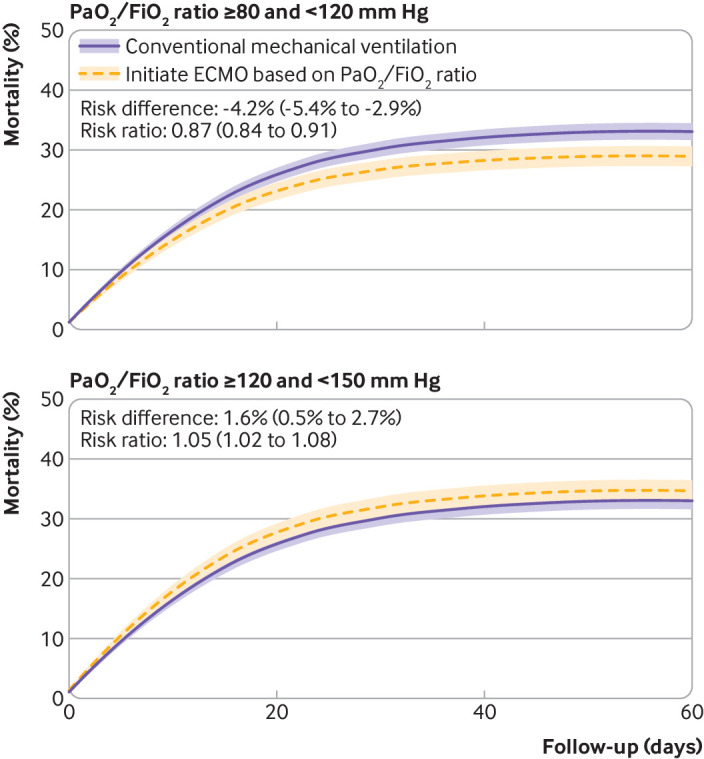
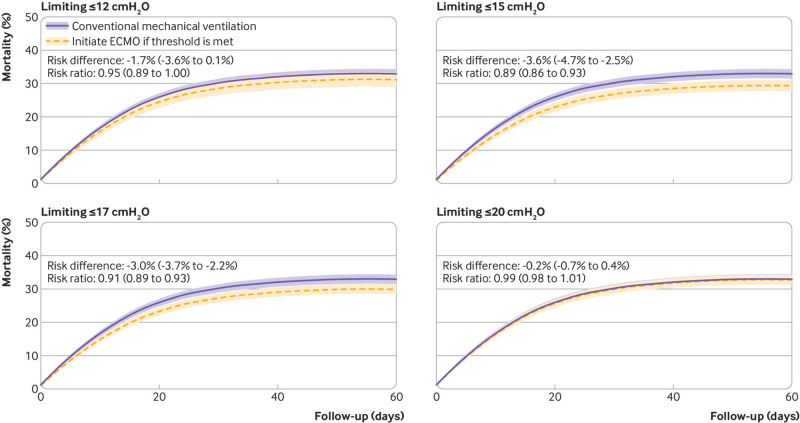
Results: 844 of 7345 eligible patients (11.5%) received ECMO at any time point during follow-up. Adherence adjusted mortality was 26.0% (95% confidence interval 24.5% to 27.5%) for a treatment strategy that included ECMO if the PaO2/FiO2 ratio decreased <80 mm Hg compared with 33.2% (31.8% to 34.6%) had patients received conventional treatment without ECMO (risk difference -7.1%, 95% confidence interval -8.2% to -6.1%; risk ratio 0.78, 95% confidence interval 0.75 to 0.82). In secondary analyses, ECMO was most effective in patients aged <65 years and with a PaO2/FiO2 <80 mm Hg or with driving pressures >15 cmH2O during the first 10 days of mechanical ventilation.
Conclusions: ECMO was associated with a reduction in mortality in selected adults with covid-19 associated respiratory failure. Age, severity of hypoxaemia, and duration and intensity of mechanical ventilation were found to be modifiers of treatment effectiveness and should be considered when deciding to initiate ECMO in patients with covid-19.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at https://www.icmje.org/coi_dischlosure.pdf. MU is supported by a Vanier Canada graduate scholarship from the Canadian Institutes of Health Research. AGB is supported by a National Health and Medical Research Council fellowship. SH is supported by a PhD scholarship from the Prince Charles Hospital Foundation. EF reports personal fees from ALung Technologies, Aerogen, Baxter, Boehringer-Ingelheim, GE Healthcare, Inspira, and Vasomune outside the submitted work; he is the chair of the research committee, Extracorporeal Life Support Organization (ELSO) and chair of the data committee, International ECMO Network (ECMONet). DB receives research support from ALung Technologies. He reports personal fees from Abiomed, Medtronic, Inspira, Cellenkos, and Xenios; he is the president-elect of ELSO and chair of the executive committee of ECMONet. GLB is a recipient of the Biomedicine international training research programme for excellent clinician-scientists (BITRECS) fellowship; the BITRECS project has received funding from the European Union’s Horizon 2020 research and innovation programme under the Marie Skłodowska-Curie (grant agreement No 754550) and from the La Caixa Foundation (ID 100010434), under agreement LCF/PR/GN18/50310006. JFF reports grant support from Fisher and Paykel Healthcare, Xenios, Getinge, Cynata, CSL Behring (Australia), and Queensland Health outside the submitted work. CLH is supported by a National Health and Medical Research Council investigator grant from Australia. KS acknowledges research support from Metro North Hospital and Health Service. JYS is supported by the Advance Queensland Fellowship from the Queensland government.
Figures
Comment in
-
Target trial emulation: applying principles of randomised trials to observational studies.BMJ. 2022 Aug 30;378:e071108. doi: 10.1136/bmj-2022-071108. BMJ. 2022. PMID: 36041749 No abstract available.
References
-
- Peek GJ, Mugford M, Tiruvoipati R, et al. CESAR trial collaboration . Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet 2009;374:1351-63. 10.1016/S0140-6736(09)61069-2. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous