

Pathophysiology, phenotypes and management of type 2 diabetes mellitus in Indian and Chinese populations
- PMID: 35508700
- PMCID: PMC9067000
- DOI: 10.1038/s41574-022-00669-4
Pathophysiology, phenotypes and management of type 2 diabetes mellitus in Indian and Chinese populations
Abstract
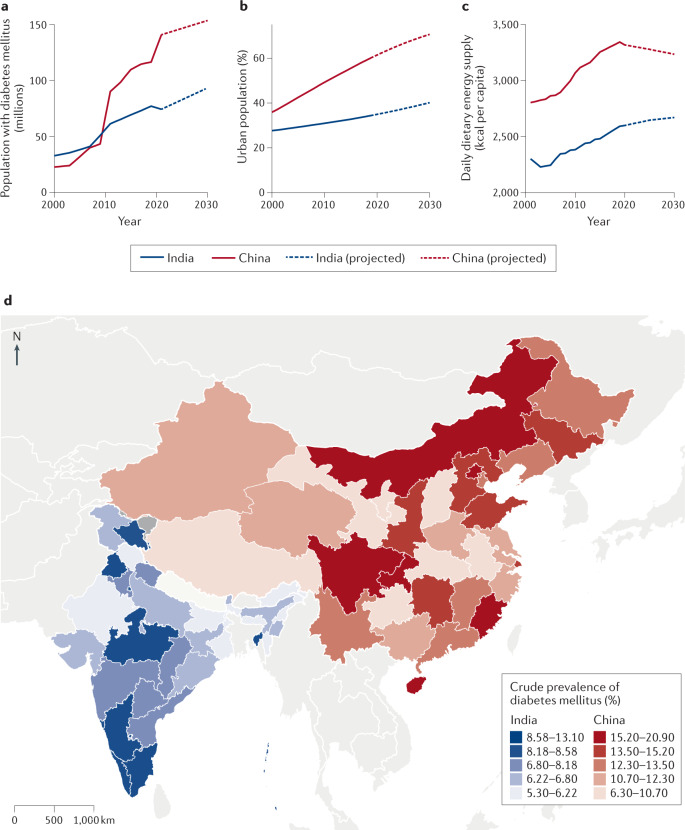
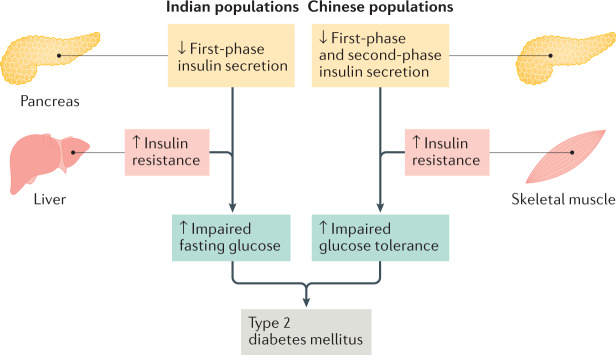
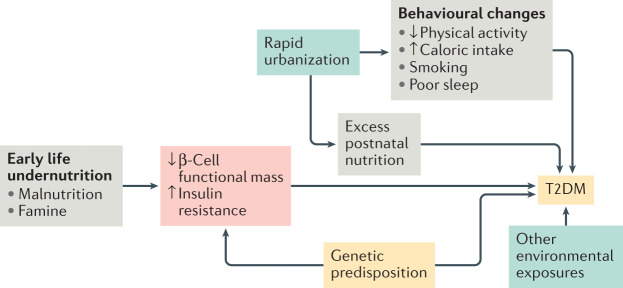
Nearly half of all adults with type 2 diabetes mellitus (T2DM) live in India and China. These populations have an underlying predisposition to deficient insulin secretion, which has a key role in the pathogenesis of T2DM. Indian and Chinese people might be more susceptible to hepatic or skeletal muscle insulin resistance, respectively, than other populations, resulting in specific forms of insulin deficiency. Cluster-based phenotypic analyses demonstrate a higher frequency of severe insulin-deficient diabetes mellitus and younger ages at diagnosis, lower β-cell function, lower insulin resistance and lower BMI among Indian and Chinese people compared with European people. Individuals diagnosed earliest in life have the most aggressive course of disease and the highest risk of complications. These characteristics might contribute to distinctive responses to glucose-lowering medications. Incretin-based agents are particularly effective for lowering glucose levels in these populations; they enhance incretin-augmented insulin secretion and suppress glucagon secretion. Sodium-glucose cotransporter 2 inhibitors might also lower blood levels of glucose especially effectively among Asian people, while α-glucosidase inhibitors are better tolerated in east Asian populations versus other populations. Further research is needed to better characterize and address the pathophysiology and phenotypes of T2DM in Indian and Chinese populations, and to further develop individualized treatment strategies.
© 2022. Springer Nature Limited.
Conflict of interest statement
C.K. reports consulting fees and honoraria from Sanofi, Abbott, and AstraZeneca. The other authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
