

Adiposity and risk of prostate cancer death: a prospective analysis in UK Biobank and meta-analysis of published studies
- PMID: 35509091
- PMCID: PMC9069769
- DOI: 10.1186/s12916-022-02336-x
Adiposity and risk of prostate cancer death: a prospective analysis in UK Biobank and meta-analysis of published studies
Abstract
Background: The association of adiposity with prostate cancer specific mortality remains unclear. We examined how adiposity relates to fatal prostate cancer and described the cross-sectional associations of commonly used adiposity measurements with adiposity estimated by imaging in UK Biobank. We also conducted a dose-response meta-analysis to integrate the new data with existing prospective evidence.
Methods: 218,237 men from UK Biobank who were free from cancer at baseline were included. Body mass index (BMI), total body fat percentage (using bioimpedance), waist circumference (WC) and waist-to-hip ratio (WHR) were collected at recruitment. Risk of dying from prostate cancer (primary cause) by the different adiposity measurements was estimated using multivariable-adjusted Cox proportional hazards models. Results from this and other prospective cohort studies were combined in a dose-response meta-analysis.
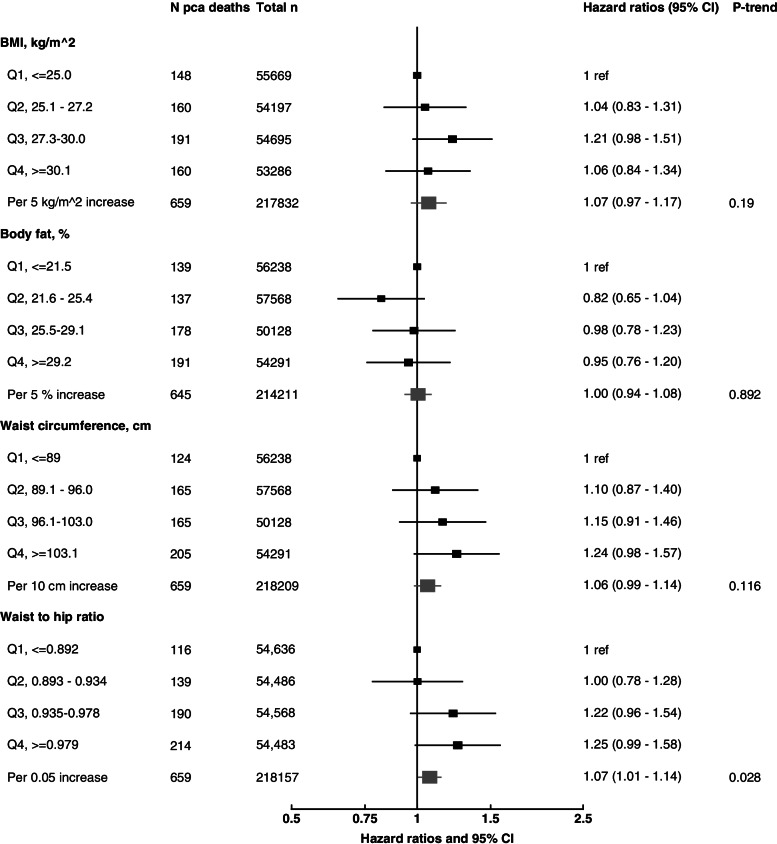
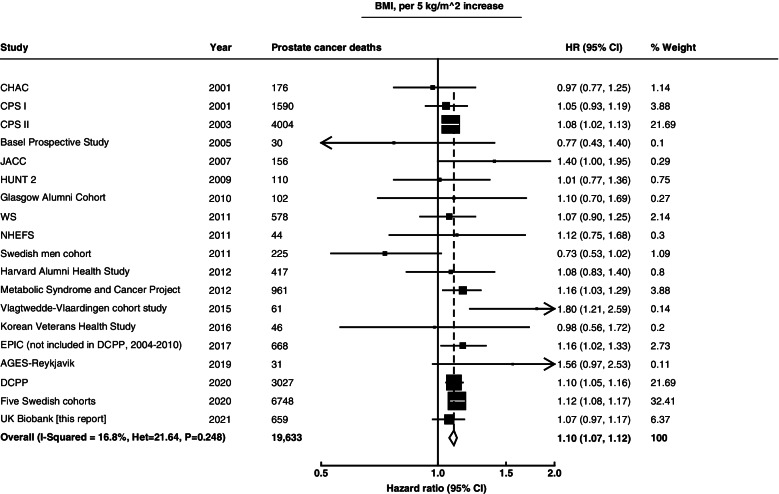
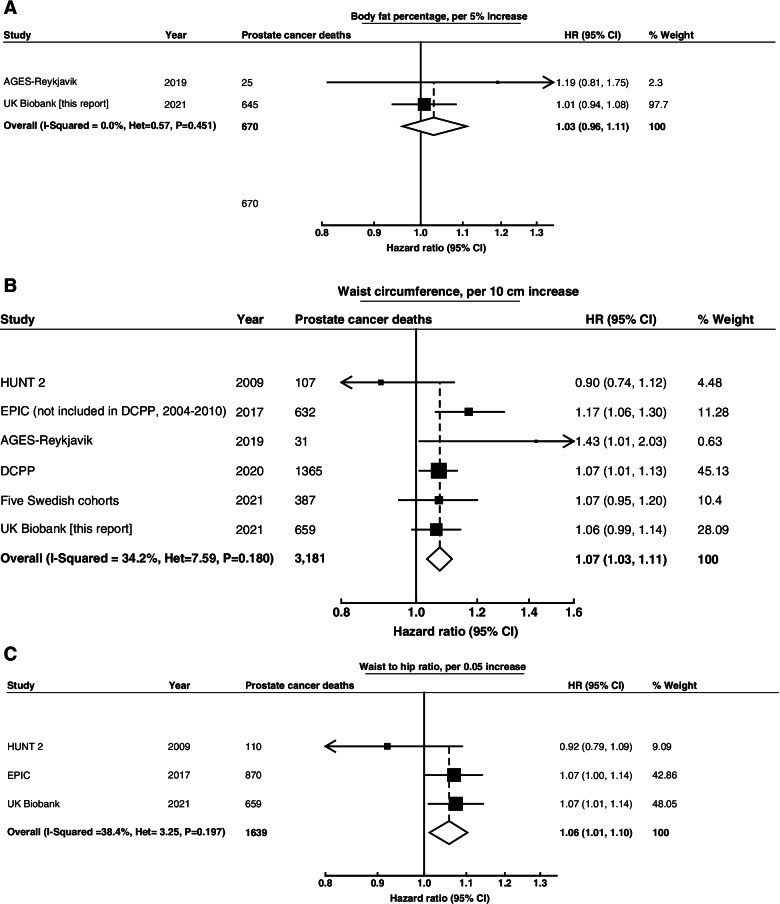
Results: In UK Biobank, 661 men died from prostate cancer over a mean follow-up of 11.6 years. In the subsample of participants with magnetic resonance imaging and dual-energy X-ray absorptiometry, BMI, body fat percentage and WC were strongly associated with imaging estimates of total and central adiposity (e.g. visceral fat, trunk fat). The hazard ratios (HR) for prostate cancer death were 1.07 (95% confidence interval = 0.97-1.17) per 5 kg/m2 higher BMI, 1.00 (0.94-1.08) per 5% increase in total body fat percentage, 1.06 (0.99-1.14) per 10 cm increase in WC and 1.07 (1.01-1.14) per 0.05 increase in WHR. Our meta-analyses of prospective studies included 19,633 prostate cancer deaths for BMI, 670 for body fat percentage, 3181 for WC and 1639 for WHR, and the combined HRs for dying from prostate cancer for the increments above were 1.10 (1.07-1.12), 1.03 (0.96-1.11), 1.07 (1.03-1.11), and 1.06 (1.01-1.10), respectively.
Conclusion: Overall, we found that men with higher total and central adiposity had similarly higher risks of prostate cancer death, which may be biologically driven and/or due to differences in detection. In either case, these findings support the benefit for men of maintaining a healthy body weight.
Keywords: Adiposity; Imaging; Mortality; Population-attributable risk; Prostate cancer.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- WCRF/AICR. World Cancer Research Fund International/American Institute for Cancer Research Continuous Update Project Report: Diet, Nutrition, Physical Activity, and Prostate Cancer. Available at: http://www.wcrf.org/sites/default/files/Prostate-Cancer-SLR-2014.pdf. 2014.
-
- Watts EL, Fensom GK, Smith Byrne K, Perez-Cornago A, Allen NE, Knuppel A, et al. Circulating insulin-like growth factor-I, total and free testosterone concentrations and prostate cancer risk in 200 000 men in UK Biobank. Int J Cancer. 2021;148(9):2274–2288. doi: 10.1002/ijc.33416. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
