

Lynch syndrome testing of colorectal cancer patients in a high-income country with universal healthcare: a retrospective study of current practice and gaps in seven australian hospitals
- PMID: 35509103
- PMCID: PMC9066828
- DOI: 10.1186/s13053-022-00225-1
Lynch syndrome testing of colorectal cancer patients in a high-income country with universal healthcare: a retrospective study of current practice and gaps in seven australian hospitals
Abstract
Background: To inform effective genomic medicine strategies, it is important to examine current approaches and gaps in well-established applications. Lynch syndrome (LS) causes 3-5% of colorectal cancers (CRCs). While guidelines commonly recommend LS tumour testing of all CRC patients, implementation in health systems is known to be highly variable. To provide insights on the heterogeneity in practice and current bottlenecks in a high-income country with universal healthcare, we characterise the approaches and gaps in LS testing and referral in seven Australian hospitals across three states.
Methods: We obtained surgery, pathology, and genetics services data for 1,624 patients who underwent CRC resections from 01/01/2017 to 31/12/2018 in the included hospitals.
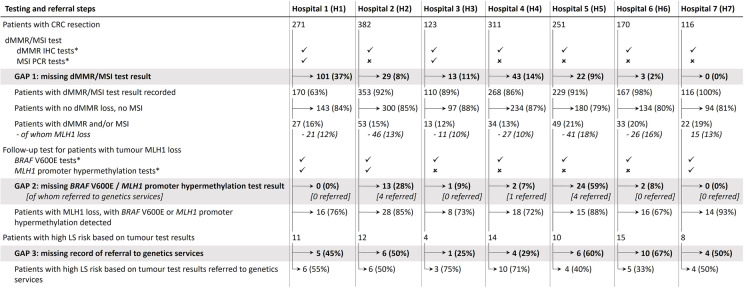
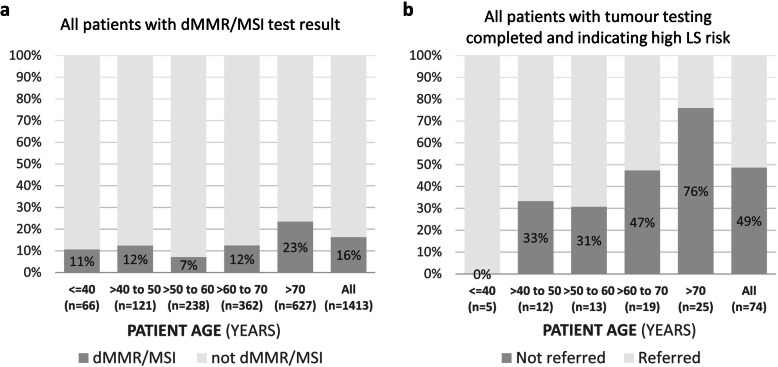
Results: Tumour testing approaches differed between hospitals, with 0-19% of patients missing mismatch repair deficiency test results (total 211/1,624 patients). Tumour tests to exclude somatic MLH1 loss were incomplete at five hospitals (42/187 patients). Of 74 patients with tumour tests completed appropriately and indicating high risk of LS, 36 (49%) were missing a record of referral to genetics services for diagnostic testing, with higher missingness for older patients (0% of patients aged ≤ 40 years, 76% of patients aged > 70 years). Of 38 patients with high-risk tumour test results and genetics services referral, diagnostic testing was carried out for 25 (89%) and identified a LS pathogenic/likely pathogenic variant for 11 patients (44% of 25; 0.7% of 1,624 patients).
Conclusions: Given the LS testing and referral gaps, further work is needed to identify strategies for successful integration of LS testing into clinical care, and provide a model for hereditary cancers and broader genomic medicine. Standardised reporting may help clinicians interpret tumour test results and initiate further actions.
Keywords: Bottleneck; Gap; Genetics services referral; Heterogeneity in practice; Lynch syndrome; Medical records; Mismatch repair; Tumour testing.
© 2022. The Author(s).
Conflict of interest statement
KC is co-PI of unrelated investigator-initiated trial of cervical screening in Australia (‘Compass’) conducted by the Victorian Cytology Service, which has received funding contribution from Roche Molecular Systems and Ventana, USA. The other authors declare no potential conflicts of interest.
Figures
Similar articles
-
Systems approach to enhance Lynch syndrome diagnosis through tumour testing.J Med Genet. 2023 Jun;60(6):533-539. doi: 10.1136/jmg-2022-108770. Epub 2022 Sep 17. J Med Genet. 2023. PMID: 36115663 Free PMC article.
-
Rates and outcomes of testing for lynch syndrome in a national colorectal cancer screening programme.Cancer Epidemiol. 2023 Feb;82:102314. doi: 10.1016/j.canep.2022.102314. Epub 2023 Jan 4. Cancer Epidemiol. 2023. PMID: 36608496
-
Impact of universal immunohistochemistry on Lynch syndrome diagnosis in an Australian colorectal cancer cohort.Intern Med J. 2019 Oct;49(10):1278-1284. doi: 10.1111/imj.14230. Intern Med J. 2019. PMID: 30667141
-
Comparison of universal screening in major lynch-associated tumors: a systematic review of literature.Fam Cancer. 2022 Jan;21(1):57-67. doi: 10.1007/s10689-020-00226-w. Epub 2021 Jan 11. Fam Cancer. 2022. PMID: 33426601
-
DNA Mismatch Repair Deficiency Tumour Testing for Patients With Colorectal Cancer: A Health Technology Assessment [Internet].Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2016 Aug. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2016 Aug. PMID: 27631047 Free Books & Documents. Review.
Cited by
-
Using a multistep approach with multidisciplinary team to increase the diagnosis rate of Lynch syndrome-associated colorectal cancer after universal screening: a single-center study in Japan.Hered Cancer Clin Pract. 2023 Jul 17;21(1):14. doi: 10.1186/s13053-023-00258-0. Hered Cancer Clin Pract. 2023. PMID: 37460934 Free PMC article.
-
Compliance of a Tertiary Centre With Molecular Testing Strategies for Lynch Syndrome in Colorectal Cancer.Cureus. 2024 Nov 11;16(11):e73475. doi: 10.7759/cureus.73475. eCollection 2024 Nov. Cureus. 2024. PMID: 39529921 Free PMC article.
-
In person and virtual process mapping experiences to capture and explore variability in clinical practice: application to genetic referral pathways across seven Australian hospital networks.Transl Behav Med. 2023 Aug 11;13(8):561-570. doi: 10.1093/tbm/ibad009. Transl Behav Med. 2023. PMID: 37036763 Free PMC article.
-
Trials and tribulations: a qualitative exploration of researcher perspectives on navigating the challenges of health system implementation research.BMJ Open. 2025 Jan 15;15(1):e087926. doi: 10.1136/bmjopen-2024-087926. BMJ Open. 2025. PMID: 39819940 Free PMC article.
References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians; 2021. - PubMed
-
- U.S National Library of Medicine. Lynch Syndrome 2021. 2020. https://ghr.nlm.nih.gov/condition/lynch-syndrome. Accessed 20 Apr 2022.
-
- Evaluation of Genomic Applications in P, Prevention Working Group Recommendations from the EGAPP Working Group: genetic testing strategies in newly diagnosed individuals with colorectal cancer aimed at reducing morbidity and mortality from Lynch syndrome in relatives. Genet Med. 2009;11(1):35–41. doi: 10.1097/GIM.0b013e31818fa2ff. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
