

RSV-associated hospitalization in adults in the USA: A retrospective chart review investigating burden, management strategies, and outcomes
- PMID: 35509398
- PMCID: PMC9059216
- DOI: 10.1002/hsr2.556
RSV-associated hospitalization in adults in the USA: A retrospective chart review investigating burden, management strategies, and outcomes
Abstract
Background and aims: The burden of respiratory syncytial virus (RSV) infection in adults is of growing concern. This study was designed to quantify disease burden, treatment approaches, and outcomes associated with RSV infections in adult subpopulations, from prehospitalization to hospital discharge.
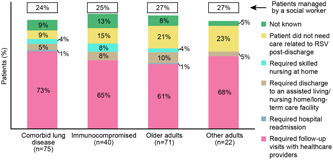
Methods: A retrospective chart analysis was conducted to collect patient-case data from hospitalized US adults (aged >18 years) with RSV infection during two RSV seasons. Patients were categorized into risk groups: comorbid lung disease, immunocompromised, older adults (aged ≥65 years), and other adults (aged <65 years). Physicians reported diagnosis, treatment choices including respiratory supportive therapy (oxygen and fluid supplementation), and outcome variables using a standardized online case form.
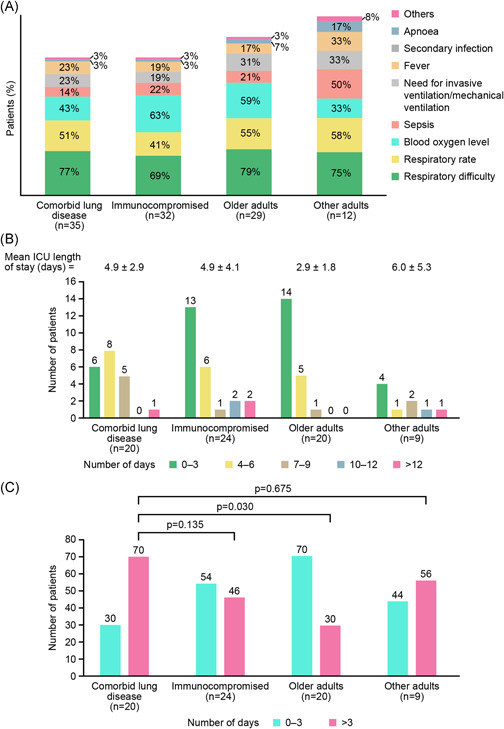
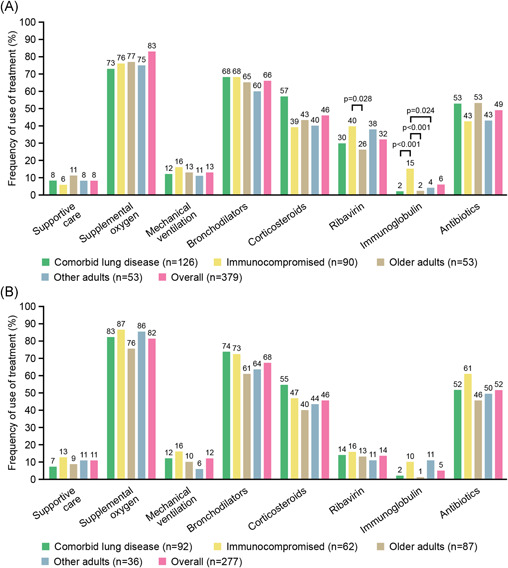
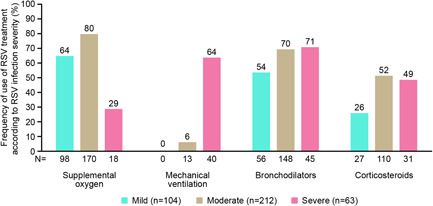
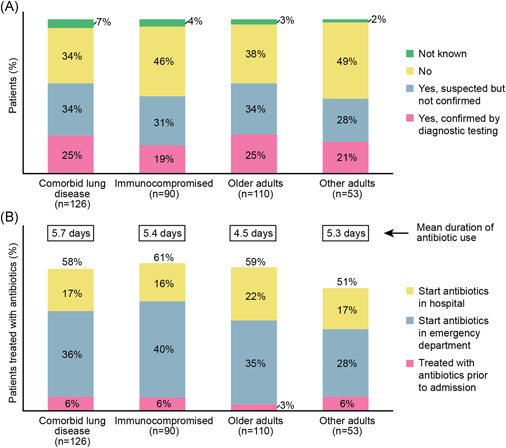
Results: The majority (277/379; 73%) of patients presented to the emergency room, with a mean age of 60 years. Once hospitalized, the median length of stay was 6.0 days (3.0-9.0), with disease severity having the greatest impact on duration of stay. No significant between-group differences in rates of patients requiring management in intensive care units were found (comorbid lung disease, 28%; immunocompromised, 36%; older adults, 26%; and other adults, 23%). Overall, respiratory supportive therapy was the most commonly used form of treatment. Antibiotics were administered in over half of all risk groups (comorbid lung disease, 61%; immunocompromised, 59%; older adults, 59%; and other adults, 51%). Patients usually required follow-up visits following discharge, with 10%-16% requiring skilled nursing care and approximately 25% requiring assistance from a social worker.
Conclusion: RSV in adult subpopulations, irrespective of age, is a significant burden to healthcare systems.
Keywords: adult; burden of disease; respiratory syncytial virus; retrospective.
© 2022 The Authors. Health Science Reports published by Wiley Periodicals LLC.
Conflict of interest statement
Nelson Lee has previously received honoraria for consultancy work, speaking in educational programs, and/or travel support from Shionogi Inc., Janssen, Sanofi Pasteur Ltd., F. Hoffmann‐La Roche Ltd., Genentech Inc., CIDARA Therapeutics Inc. Edward Walsh has research contracts from Gilead, Janssen, Merck Sharp & Dohme and unpaid consultation to Novavax, and Pfizer. Robert Stolper and Jessica Zakar are employees of IQVIA, a healthcare consulting firm engaged by Janssen Pharmaceuticals. Ian Sander is a former employee of IQVIA and a current employee of Ironwood Pharmaceuticals. Veronique Wyffels and Roman Fleischhackl are employees of Janssen Pharmaceuticals. David Myers is a former employee of Janssen Pharmaceuticals. Veronique Wyffels and Roman Fleischhackl may be Johnson & Johnson stockholders.
Figures
References
-
- Walsh EE, Falsey AR. Respiratory syncytial virus infection in adult populations. Infect Disord Drug Targets. 2012;12(2):98‐102. - PubMed
-
- Pilie P, Werbel WA, Riddell J, Shu X, Schaubel D, Gregg KS 4th. Adult patients with respiratory syncytial virus infection: impact of solid organ and hematopoietic stem cell transplantation on outcomes. Transpl Infect Dis. 2015;17(4):551‐557. - PubMed
-
- Falsey AR, Hennessey PA, Formica MA, Cox C, Walsh EE. Respiratory syncytial virus infection in elderly and high‐risk adults. N Engl J Med. 2005;352(17):1749‐1759. - PubMed
LinkOut - more resources
Full Text Sources
