

Impact of delay from transperineal biopsy to radical prostatectomy upon objective measures of cancer control
- PMID: 35509478
- PMCID: PMC9051344
- DOI: 10.1016/j.ajur.2021.08.008
Impact of delay from transperineal biopsy to radical prostatectomy upon objective measures of cancer control
Abstract
Objective: Treatment delays in prostate cancer have been characterised, although not explicitly in men undergoing transperineal prostate biopsies. We aimed to determine if delays to radical prostatectomy correlate with adverse outcomes using a contemporary population-based cohort of men diagnosed by transperineal biopsies.
Methods: This study analysed men with prostate cancer of the International Society for Urological Pathology grade group ≥2, diagnosed by transperineal prostate biopsies who underwent prostatectomy, using the prospectively data from 1 January 2014 to 30 June 2018 Prostate Cancer Outcomes Registry-Victoria. Data were analysed according to stratified demographic and disease characteristics. Time intervals from biopsy (28, 60, 90, 120, and 270 days) were compared using odds ratios and regression analyses for proportion of upgrading, early biochemical recurrence, pT3 disease at prostatectomy, and positive surgical margins.
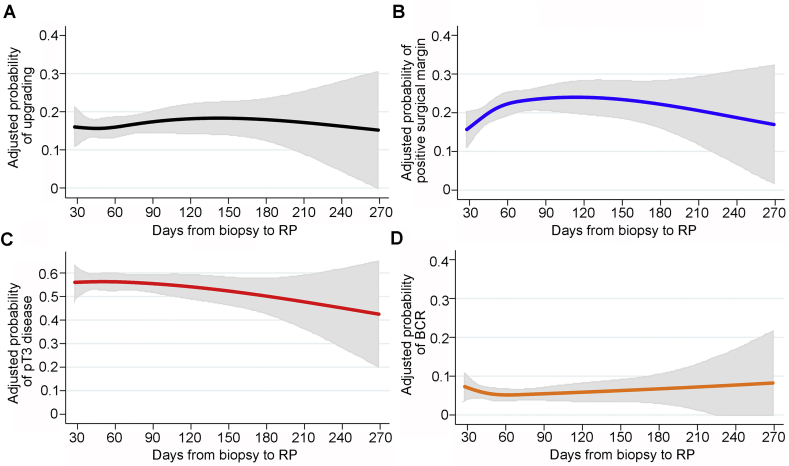
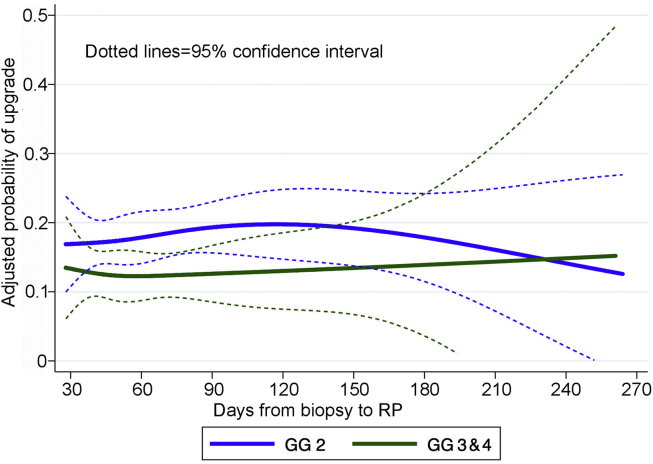
Results: In total, 2008 men were analysed. There were 306 (16.7%) men with upgrading, 151 (8.4%) with biochemical recurrence, 1068 (54.1%) with pT3 disease, and 464 (23.1%) with positive surgical margins (percentages excluded patients with missing data). All adverse outcomes studied were significantly associated with higher prostate-specific antigen and grade at diagnosis. Delays of 120-270 days did not adversely alter the incidence of Gleason upgrading, pT3, or recurrence. Delays (most frequent 60-89 days, 28%) were associated with positive surgical margins but not monotonically. Regression modelling demonstrated no increased likelihood of most adverse outcomes for up to 270 days.
Conclusion: Men with prostate cancer of grade group ≥2 diagnosed through transperineal biopsy may wait up to 270 days for a prostatectomy without a greater likelihood of upgrading, pT3 disease, positive surgical margins, or biochemical recurrence.
Keywords: Biopsy; Disease progression; Prostate cancer; Recurrence; Treatment delay.
© 2022 Editorial Office of Asian Journal of Urology. Production and hosting by Elsevier B.V.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
The effect of time from biopsy to radical prostatectomy on adverse pathologic outcomes.Res Rep Urol. 2019 Mar 6;11:53-60. doi: 10.2147/RRU.S187950. eCollection 2019. Res Rep Urol. 2019. PMID: 30881945 Free PMC article.
-
Delay from biopsy to radical prostatectomy influences the rate of adverse pathologic outcomes.Prostate. 2015 Jul 1;75(10):1085-91. doi: 10.1002/pros.22992. Epub 2015 Mar 21. Prostate. 2015. PMID: 25809289
-
Prostate-specific antigen vs prostate-specific antigen density as a predictor of upgrading in men diagnosed with Gleason 6 prostate cancer by contemporary multicore prostate biopsy.BJU Int. 2012 Dec;110(11 Pt B):E494-9. doi: 10.1111/j.1464-410X.2012.11182.x. Epub 2012 Apr 30. BJU Int. 2012. PMID: 22540236
-
Clinical significance and risk factors of International Society of Urological Pathology (ISUP) grade upgrading in prostate cancer patients undergoing robot-assisted radical prostatectomy.BMC Cancer. 2021 May 4;21(1):501. doi: 10.1186/s12885-021-08248-y. BMC Cancer. 2021. PMID: 33947348 Free PMC article.
-
Incidence, etiology, location, prevention and treatment of positive surgical margins after radical prostatectomy for prostate cancer.J Urol. 1998 Aug;160(2):299-315. J Urol. 1998. PMID: 9679867 Review.
Cited by
-
Surgical Wait Time Is Not Associated With Oncological or Psychosocial Outcomes After Robotic Radical Prostatectomy.Prostate Cancer. 2025 Jul 29;2025:4314397. doi: 10.1155/proc/4314397. eCollection 2025. Prostate Cancer. 2025. PMID: 40766967 Free PMC article.
-
The association between the interval from biopsy to radical prostatectomy and biochemical recurrence in patients with intermediate- and high-risk prostate cancer.Front Oncol. 2025 Feb 4;14:1533800. doi: 10.3389/fonc.2024.1533800. eCollection 2024. Front Oncol. 2025. PMID: 39968383 Free PMC article.
References
-
- Bray F., Ferlay J., Soerjomataram I., Siegel R.L., Torre L.A., Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. - PubMed
-
- Mottet N., Bellmunt J., Bolla M., Briers E., Cumberbatch M.G., De Santis M., et al. EAU-ESTRO-SIOG guidelines on prostate cancer. Part 1: Screening, diagnosis, and local treatment with curative intent. Eur Urol. 2017;71:618–629. - PubMed
-
- Ginsburg K.B., Curtis G.L., Timar R.E., George A.K., Cher M.L. Delayed radical prostatectomy is not associated with adverse oncological outcomes: Implications for men experiencing surgical delay due to the COVID-19 pandemic. J Urol. 2020;204:720–725. - PubMed
-
- Bianchi L., Schiavina R., Borghesi M., Casablanca C., Chessa F., Mineo Bianchi F., et al. Patterns of positive surgical margins after open radical prostatectomy and their association with clinical recurrence. Minerva Urol Nefrol. 2020;72:464–473. - PubMed
LinkOut - more resources
Full Text Sources
