

Mortality, healthcare resource utilization, and cost among Medicare beneficiaries with Clostridioides difficile infection with and without sepsis
- PMID: 35510091
- PMCID: PMC9058456
- DOI: 10.1177/20499361221095679
Mortality, healthcare resource utilization, and cost among Medicare beneficiaries with Clostridioides difficile infection with and without sepsis
Abstract
Objective: To describe mortality, healthcare resource utilization (HRU), and costs among Medicare beneficiaries with primary Clostridioides difficile infection (pCDI) or recurrent CDI (rCDI), with and without sepsis.
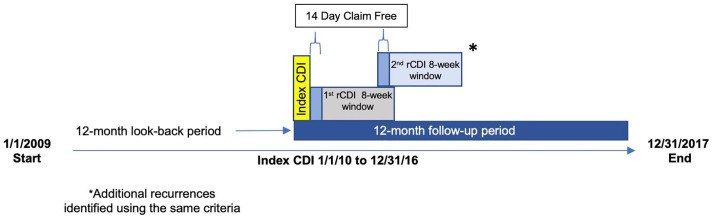
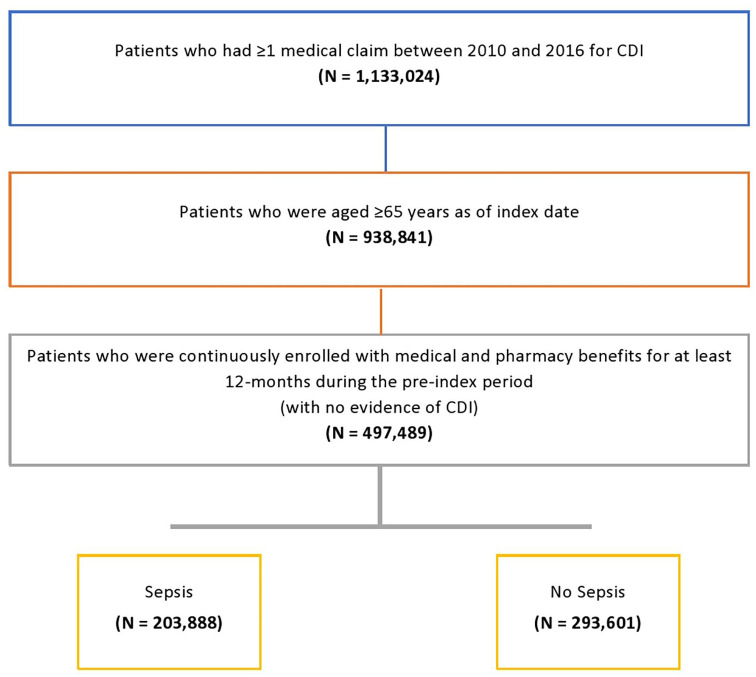
Methods: We conducted a retrospective observational study of 100% Medicare Fee-for-Service claims from adults aged ⩾ 65 years with ⩾1 CDI episode between 1 January 2009 and 31 December 2017. Patients were continuously enrolled in Medicare Parts A/B/D 12 months before and up to 12 months after pCDI. ICD-9/10 codes defined CDI using ⩾1 inpatient claim, or ⩾1 outpatient claim plus ⩾1 claim for CDI treatment. The pCDI episode ended after 14 days without a CDI claim. rCDI episodes started within 8 weeks from the end of a previous CDI episode. ICD-9/10 codes identified all-cause sepsis over 12 month follow-up.
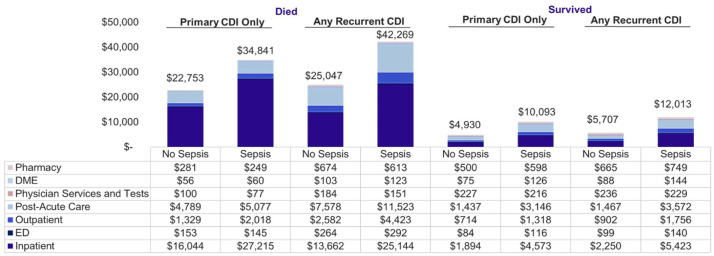
Results: Of 497,489 CDI patients, 41.0% (N = 203,888) had sepsis; 57.7% with sepsis died versus 32.4% without sepsis. Among patients with pCDI only (N = 345,893) or ⩾1 rCDI (N = 151,596), 39.2% and 45.1% suffered sepsis, respectively. All-cause hospitalizations were frequent for all cohorts (range: 81-99%). Among patients who died, those with sepsis versus without had more-frequent intensive care unit (ICU) use (pCDI: 29% versus 15%; rCDI: 65% versus 34%), longer hospital stays (pCDI: 12 versus 10 days; rCDI: 12 versus 9 days), and higher per-patient-per-month costs (pCDI: $34,841 versus $22,753; rCDI: $42,269 versus $25,047). In both cohorts, sepsis patients who survived had higher total costs and all-cause HRU than those without sepsis. All p < 0.001 above.
Conclusions: Sepsis was common among Medicare beneficiaries with CDI. CDI patients with sepsis, especially after an rCDI, experienced higher mortality, HRU, and costs compared with those without sepsis.
Keywords: Clostridioides difficile; Clostridium difficile infection; Medicare; cost; healthcare resource utilization; recurrent CDI; sepsis.
© The Author(s), 2022.
Conflict of interest statement
Conflict of interest statement: The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DD and WWN were employees of Ferring Pharmaceuticals at the time of the research and manuscript development. IM and CT are employees of Avalere Health. JD and AW were employees of Avalere Health at the time of the research and manuscript development. PF: Merck and Co.: Speakers Bureau; Ferring/Rebiotix: Consulting, Advisory Board; SERES Therapeutics: Advisory Board; Takeda Pharmaceuticals: Advisory Board. AA: PI or co-I of clinical trials sponsored by NIH/NIAID, NeuroRx Pharma, Pulmotect, Blade Therpeutics, Novartis, Takeda, Humanigen, Eli Lilly, PTC Therapeutics, OctaPharma, Fulcrum Therapeutics, Alexion. He has served as a speaker and/or consultant for BMS, Pfizer, BI, Portola, Sunovion, Mylan, Salix, Alexion, AstraZeneca, Novartis, Nabriva, Paratek, Bayer, Tetraphase, Achogen LaJolla, Ferring, Seres, Millenium, HeartRite, Aseptiscope, Sprightly.
Figures
References
-
- Ma GK, Brensinger CM, Wu Q, et al.. Increasing incidence of multiply recurrent Clostridium difficile infection in the United States: a cohort study. Ann Intern Med 2017; 167: 152–158. - PubMed
-
- Johnson S. Recurrent Clostridium difficile infection: causality and therapeutic approaches. Int J Antimicrob Agents 2009; 33(Suppl. 1): S33–S36. - PubMed
