

Clinical use of expanded prostate cancer index composite-based health-related quality of life outcomes after robot-assisted radical prostatectomy for localized prostate cancer
- PMID: 35510095
- PMCID: PMC9042679
- DOI: 10.1016/j.prnil.2021.08.001
Clinical use of expanded prostate cancer index composite-based health-related quality of life outcomes after robot-assisted radical prostatectomy for localized prostate cancer
Abstract
Background: This study aimed to assess the longitudinal health-related quality of life (HRQOL) using the Expanded Prostate Cancer Index Composite (EPIC) and HRQOL change between the nerve-sparing technique in Japanese men treated with robot-assisted radical prostatectomy (RARP).
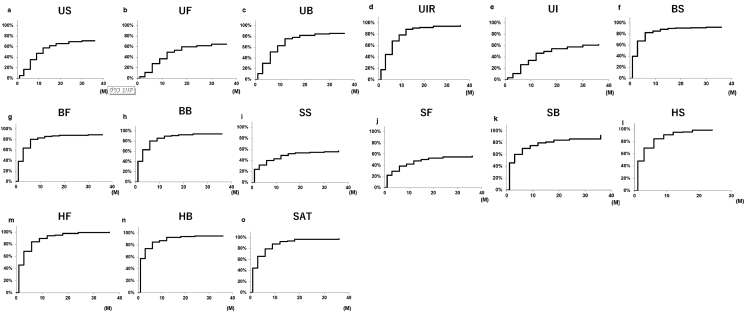
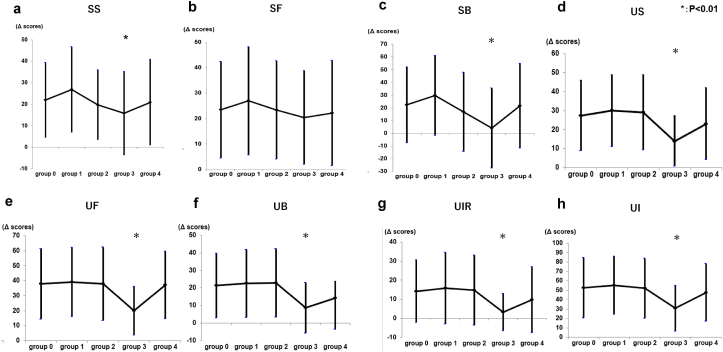
Methods: A total of 573 patients who received RARP were included in this study. EPIC questionnaire was administered before treatment and up to 36 months after RARP. Clinical recovery was defined as half of the standard deviation of the baseline score for each domain. We divided all patients into recovery group or nonrecovery group. The time from survey to each domain recovery was calculated using the Kaplan-Meier method. We compared the sexual and urinary score change between groups using analysis of variance to confirm the effect of nerve-sparing technique.
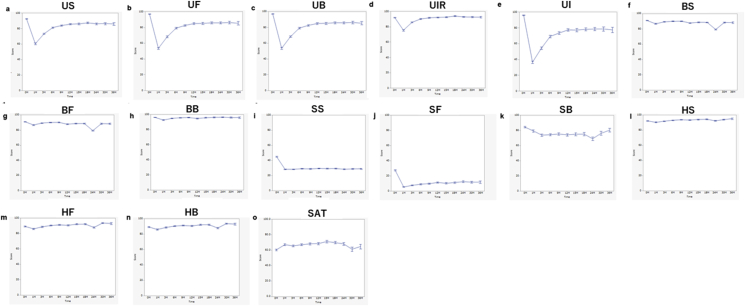
Results: The median age was 67 years (interquartile range, 62-71 years). The mean score of all urinary domains worsened noticeably after 1 month. All postoperative urinary summary, function, and incontinence scores were significantly lower than preoperative scores up to 3 years post-RARP. Postoperative sexual summary and functional scores were significantly lower than preoperative score at all follow-up times throughout the 36 months. The recovery rate for the urinary incontinence domain was the lowest (44.5%), whereas the recovery rate for the urinary irritative-obstructive domain was the highest (73.7%). In the sexual domain, the bother domain had a higher recovery rate (73.0%) than the functional domain (29.7%). Although the recovery of sexual domains was slower compared with other domains, by 36 months after RARP, almost all values had recovered. Compared with other technique groups, bilateral intrafascial nerve-sparing group showed significantly decreased change in subscale scores before and after RARP in several sexual and urinary domain.
Conclusion: The time course and extent of functional and bother domain recovery documented in this study may prove useful for RARP patient selection in Japan.
Keywords: Nerve-sparing surgery; Prostate cancer; Quality of life; Robot-assisted radical prostatectomy.
© 2022 Asian Pacific Prostate Society. Publishing services by Elsevier B.V.
Conflict of interest statement
None of the contributing authors have any conflicts of interest, including specific financial interests, relationships, and affiliations relevant to the subject matter or materials discussed in the article.
Figures
References
-
- Wakao F., Higashi T., Katanoda K. Foundation for Promotion of Cancer Research; Tokyo: 2018. Cancer statistics in Japan 2017.http://ganjoho.jp/data/reg_stat/statistics/brochure/2017/cancer_statisti...http://ganjoho.jp/data/reg_stat/statistics/brochure/2017/cancer_statisti... [Internet] [cited 2018 Dec 22]. Available from:
-
- Walz J., Gallina A., Saad F., Montorsi F., Perrotte P., Shariat S.F., et al. A nomogram predicting 10-year life expectancy in candidates for radical prostatectomy or radiotherapy for prostate cancer. J Clin Oncol. 2007;25:3576–3581. - PubMed
-
- Ficarra V., Novara G., Ahlering T.E., Costello A., Eastham J.A., Graefen M., et al. Systematic review and meta-analysis of studies reporting potency rates after robot-assisted radical prostatectomy. Eur Urol. 2012;62:418–430. - PubMed
-
- Wei J.T., Dunn R.L., Sandler H.M., McLaughlin P.W., Montie J.E., Litwin M.S., et al. Comprehensive comparison of health-related quality of life after contemporary therapies for localized prostate cancer. J Clin Oncol. 2002;20:557–566. - PubMed
-
- Johansson E., Steineck G., Holmberg L., Johansson J.E., Nyberg T., Ruutu M., et al. Long-term quality-of-life outcomes after radical prostatectomy or watchful waiting: the Scandinavian Prostate Cancer Group-4 randomised trial. Lancet Oncol. 2011;12:891–899. - PubMed
LinkOut - more resources
Full Text Sources