

Glucocorticoid-induced adrenal insufficiency: an uncommon cause of hypercalcaemia
- PMID: 35510507
- PMCID: PMC9175604
- DOI: 10.1530/EDM-21-0177
Glucocorticoid-induced adrenal insufficiency: an uncommon cause of hypercalcaemia
Abstract
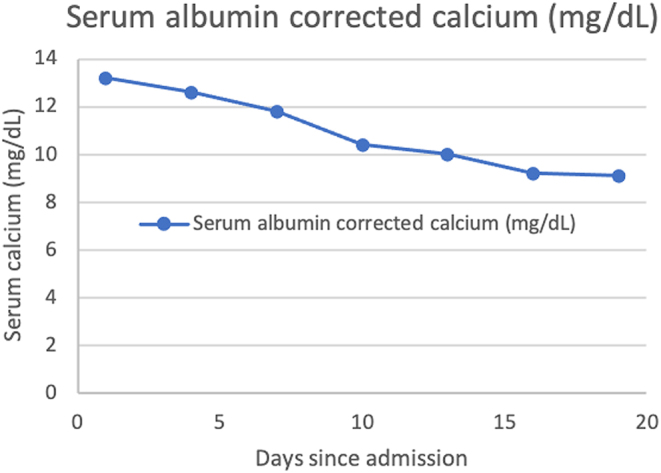
Summary: Long-term use of exogenous glucocorticoids leads to the suppression of the hypothalamic-pituitary-adrenal axis. Therefore, if the glucocorticoid is withdrawn abruptly, patients will develop adrenal insufficiency. Hypercalcaemia is a rare but well-known complication of adrenal insufficiency. However, hypercalcaemia is a rare presentation of glucocorticoid-induced adrenal insufficiency (GI-AI). A 62-year-old patient with a past history of diabetes mellitus, ischaemic heart disease, stroke, hypertension and dyslipidaemia presented with polyuria, loss of appetite, malaise and vomiting for a duration of 2 months. His ionized calcium level was high at 1.47 mmol/L. Intact parathyroid hormone was suppressed (4.3 pg/mL) and vitamin D was in the insufficient range (24.6 ng/mL). Extensive evaluation for solid organ or haematological malignancy including contrast-enhanced CT chest, abdomen, pelvis, multiple myeloma workup and multiple tumour markers were negative. His synacthan-stimulated cortisol was undetectable thus confirming adrenal insufficiency. His adrenocorticotrophic hormone level was 3.82 pg/mL (4.7-48.8) excluding primary adrenal insufficiency. His MRI brain and other pituitary hormones were normal. Further inquiry revealed that the patient had taken over-the-counter dexamethasone on a regular basis for allergic rhinitis for more than 2 years and had stopped 2 weeks prior to the onset of symptoms. Therefore, a diagnosis of GI-AI leading to hypercalcemia was made. The patient was resuscitated with intravenous fluids and replacement doses of oral hydrocortisone were started with a plan of prolonged tailing off to allow the endogenous adrenal function to recover. His calcium normalized and he made a complete recovery.
Learning points: Long-term use of glucocorticoids leads to the suppression of the hypothalamic-pituitary-adrenal axis. If the glucocorticoid is withdrawn abruptly, patients will develop adrenal insufficiency which is known as glucocorticoid-induced adrenal insufficiency. Adrenal insufficiency should be considered in the differential diagnosis of parathyroid hormone-independent hypercalcaemia. A thorough clinical history is of paramount importance in arriving at the correct diagnosis.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
