

Circulating levels and prognostic cut-offs of sST2, hs-cTnT, and NT-proBNP in women vs. men with chronic heart failure
- PMID: 35510529
- PMCID: PMC9288762
- DOI: 10.1002/ehf2.13883
Circulating levels and prognostic cut-offs of sST2, hs-cTnT, and NT-proBNP in women vs. men with chronic heart failure
Abstract
Aims: To define plasma concentrations, determinants, and optimal prognostic cut-offs of soluble suppression of tumorigenesis-2 (sST2), high-sensitivity cardiac troponin T (hs-cTnT), and N-terminal pro-B-type natriuretic peptide (NT-proBNP) in women and men with chronic heart failure (HF).
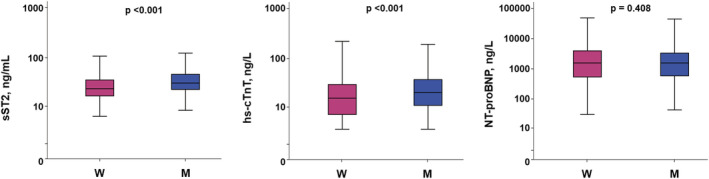
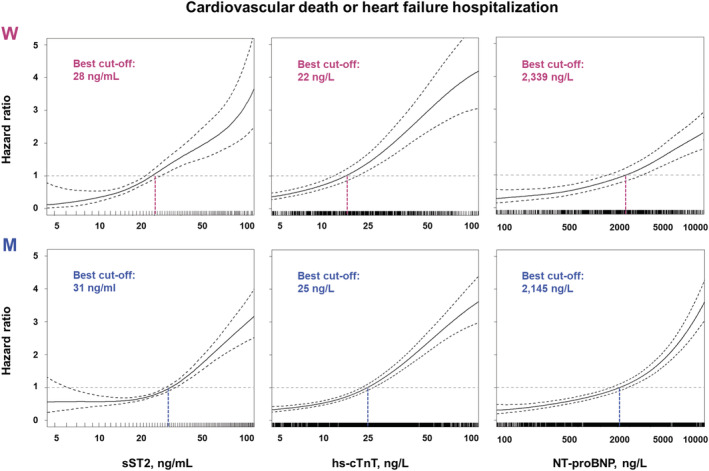
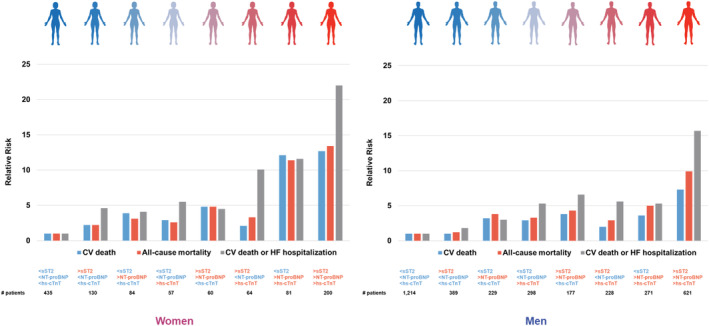
Methods and results: Individual data of patients from the Biomarkers In Heart Failure Outpatient Study (BIOS) Consortium with sST2, hs-cTnT, and NT-proBNP measured were analysed. The primary endpoint was a composite of 1 year cardiovascular death and HF hospitalization. The secondary endpoints were 5 year cardiovascular and all-cause death. The cohort included 4540 patients (age 67 ± 12 years, left ventricular ejection fraction 33 ± 13%, 1111 women, 25%). Women showed lower sST2 (24 vs. 27 ng/mL, P < 0.001) and hs-cTnT level (15 vs. 20 ng/L, P < 0.001), and similar concentrations of NT-proBNP (1540 vs. 1505 ng/L, P = 0.408). Although the three biomarkers were confirmed as independent predictors of outcome in both sexes, the optimal prognostic cut-off was lower in women for sST2 (28 vs. 31 ng/mL) and hs-cTnT (22 vs. 25 ng/L), while NT-proBNP cut-off was higher in women (2339 ng/L vs. 2145 ng/L). The use of sex-specific cut-offs improved risk prediction compared with the use of previously standardized prognostic cut-offs and allowed to reclassify the risk of many patients, to a greater extent in women than men, and for hs-cTnT than sST2 or NT-proBNP. Specifically, up to 18% men and up to 57% women were reclassified, by using the sex-specific cut-off of hs-cTnT for the endpoint of 5 year cardiovascular death.
Conclusions: In patients with chronic HF, concentrations of sST2 and hs-cTnT, but not of NT-proBNP, are lower in women. Lower sST2 and hs-cTnT and higher NT-proBNP cut-offs for risk stratification could be used in women.
Keywords: Chronic heart failure; High-sensitivity troponin T; NT-proBNP; Prognosis; Sex; Women; sST2.
© 2022 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Figures
Similar articles
-
Circulating levels and prognostic value of soluble ST2 in heart failure are less influenced by age than N-terminal pro-B-type natriuretic peptide and high-sensitivity troponin T.Eur J Heart Fail. 2020 Nov;22(11):2078-2088. doi: 10.1002/ejhf.1701. Epub 2020 Jan 9. Eur J Heart Fail. 2020. PMID: 31919929
-
Association of point-of-care testing for sST2 with clinical outcomes in patients hospitalized with heart failure.ESC Heart Fail. 2024 Oct;11(5):2857-2868. doi: 10.1002/ehf2.14860. Epub 2024 May 21. ESC Heart Fail. 2024. PMID: 38773746 Free PMC article.
-
sST2 Predicts Outcome in Chronic Heart Failure Beyond NT-proBNP and High-Sensitivity Troponin T.J Am Coll Cardiol. 2018 Nov 6;72(19):2309-2320. doi: 10.1016/j.jacc.2018.08.2165. J Am Coll Cardiol. 2018. PMID: 30384887
-
Early diagnostic value of high-sensitivity cardiac troponin T for cancer treatment-related cardiac dysfunction: a meta-analysis.ESC Heart Fail. 2023 Aug;10(4):2170-2182. doi: 10.1002/ehf2.14373. Epub 2023 May 11. ESC Heart Fail. 2023. PMID: 37170474 Free PMC article. Review.
-
High-Sensitivity Cardiac Troponin and New-Onset Heart Failure: A Systematic Review and Meta-Analysis of 67,063 Patients With 4,165 Incident Heart Failure Events.JACC Heart Fail. 2018 Mar;6(3):187-197. doi: 10.1016/j.jchf.2017.11.003. Epub 2018 Jan 10. JACC Heart Fail. 2018. PMID: 29331272
Cited by
-
Biomarkers in Heart Failure: From Research to Clinical Practice.Ann Lab Med. 2023 May 1;43(3):225-236. doi: 10.3343/alm.2023.43.3.225. Epub 2022 Dec 22. Ann Lab Med. 2023. PMID: 36544334 Free PMC article. Review.
-
Biomarkers in heart failure: Traditional and emerging indicators for prognosis.ESC Heart Fail. 2025 Jun;12(3):1535-1538. doi: 10.1002/ehf2.15168. Epub 2024 Nov 15. ESC Heart Fail. 2025. PMID: 39545304 Free PMC article. No abstract available.
-
Thromboembolic Disease and Cardiac Thrombotic Complication in COVID-19: A Systematic Review.Metabolites. 2022 Sep 22;12(10):889. doi: 10.3390/metabo12100889. Metabolites. 2022. PMID: 36295791 Free PMC article. Review.
-
Examining the Long-Term Prognostic Significance of Serum sST2: Influence of Myocardial Infarction History and Subgroup Level Standardization.J Inflamm Res. 2024 Oct 25;17:7733-7744. doi: 10.2147/JIR.S482475. eCollection 2024. J Inflamm Res. 2024. PMID: 39479262 Free PMC article.
-
Heart Failure: Is There an Ideal Biomarker?Rev Cardiovasc Med. 2023 Nov 9;24(11):310. doi: 10.31083/j.rcm2411310. eCollection 2023 Nov. Rev Cardiovasc Med. 2023. PMID: 39076445 Free PMC article. Review.
References
-
- Bloom MW, Greenberg B, Jaarsma T, Januzzi JL, Lam CSP, Maggioni AP, Trochu JN, Butler J. Heart failure with reduced ejection fraction. Nat Rev Dis Primers. 2017; 3: 17058. - PubMed
-
- Murphy SP, Ibrahim NE, Januzzi JL Jr. Heart failure with reduced ejection fraction: a review. JAMA. 2020; 324: 488–504. - PubMed
-
- Gentile F, Ghionzoli N, Borrelli C, Vergaro G, Pastore MC, Cameli M, Emdin M, Passino C, Giannoni A. Epidemiological and clinical boundaries of heart failure with preserved ejection fraction. Eur J Prev Cardiol. 2021; zwab077. - PubMed
-
- Lam CSP, Arnott C, Beale AL, Chandramouli C, Hilfiker‐Kleiner D, Kaye DM, Ky B, Santema BT, Sliwa K, Voors AA. Sex differences in heart failure. Eur Heart J. 2019; 40: 3859–3868. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
