

Cardiogenic Shock From Heart Failure Versus Acute Myocardial Infarction: Clinical Characteristics, Hospital Course, and 1-Year Outcomes
- PMID: 35510546
- PMCID: PMC9286066
- DOI: 10.1161/CIRCHEARTFAILURE.121.009279
Cardiogenic Shock From Heart Failure Versus Acute Myocardial Infarction: Clinical Characteristics, Hospital Course, and 1-Year Outcomes
Abstract
Background: Little is known about clinical characteristics, hospital course, and longitudinal outcomes of patients with cardiogenic shock (CS) related to heart failure (HF-CS) compared to acute myocardial infarction (AMI; CS related to AMI [AMI-CS]).
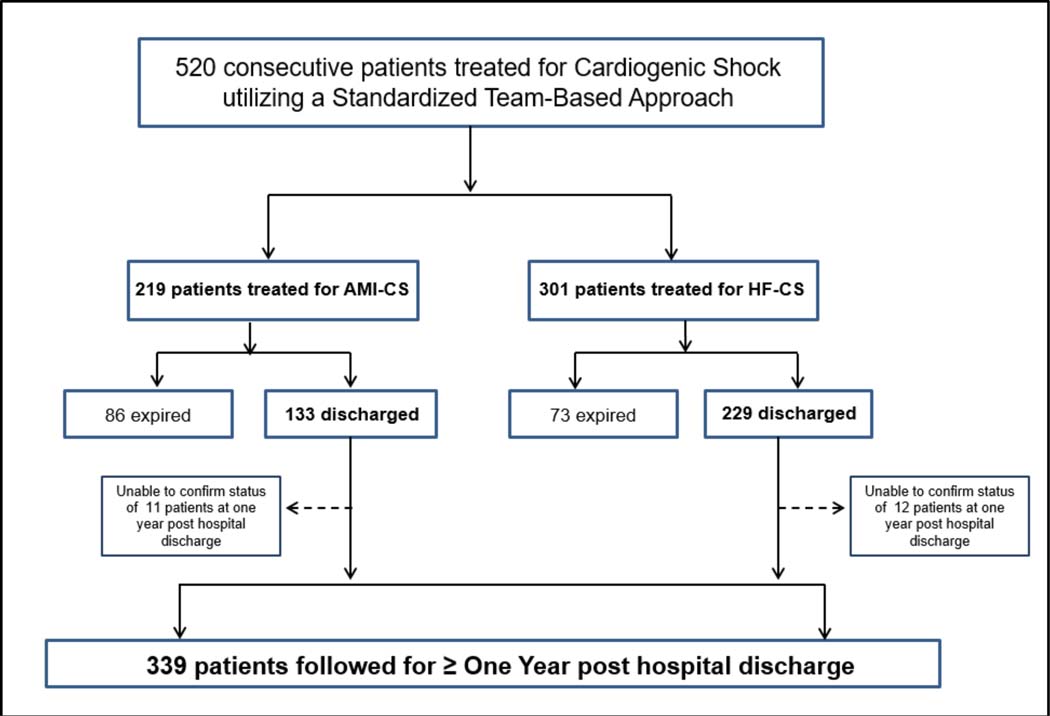
Methods: We examined in-hospital and 1-year outcomes of 520 (219 AMI-CS, 301 HF-CS) consecutive patients with CS (January 3, 2017-December 31, 2019) in a single-center registry.
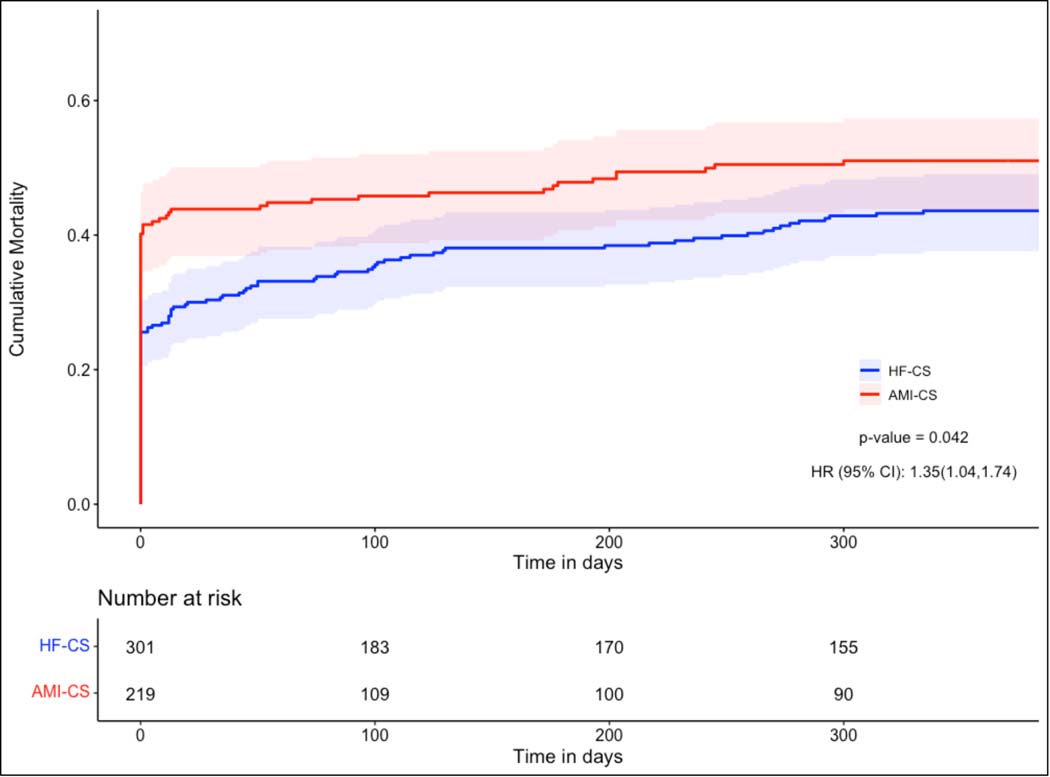
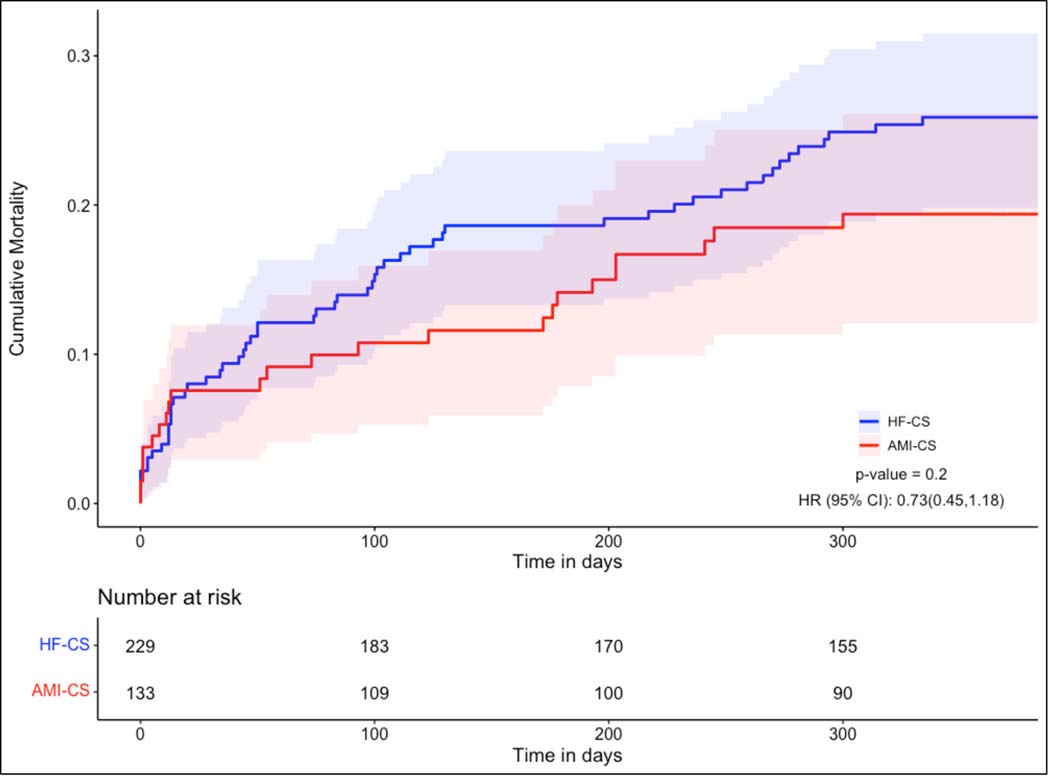
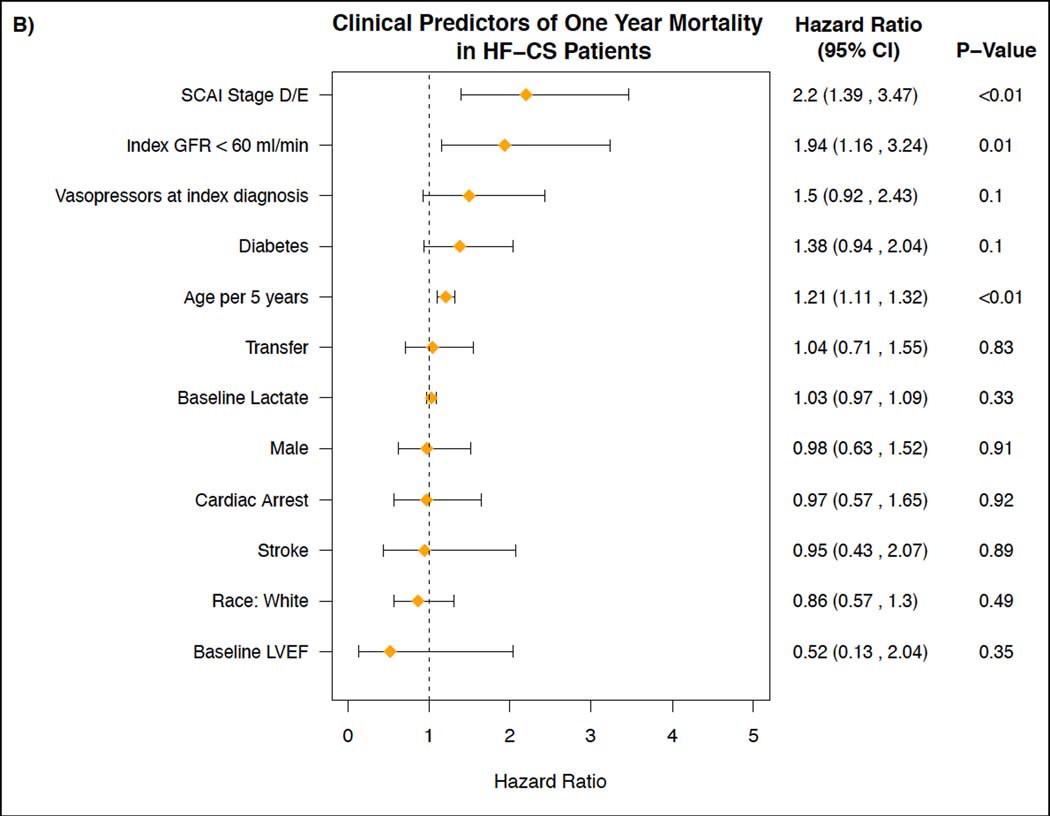
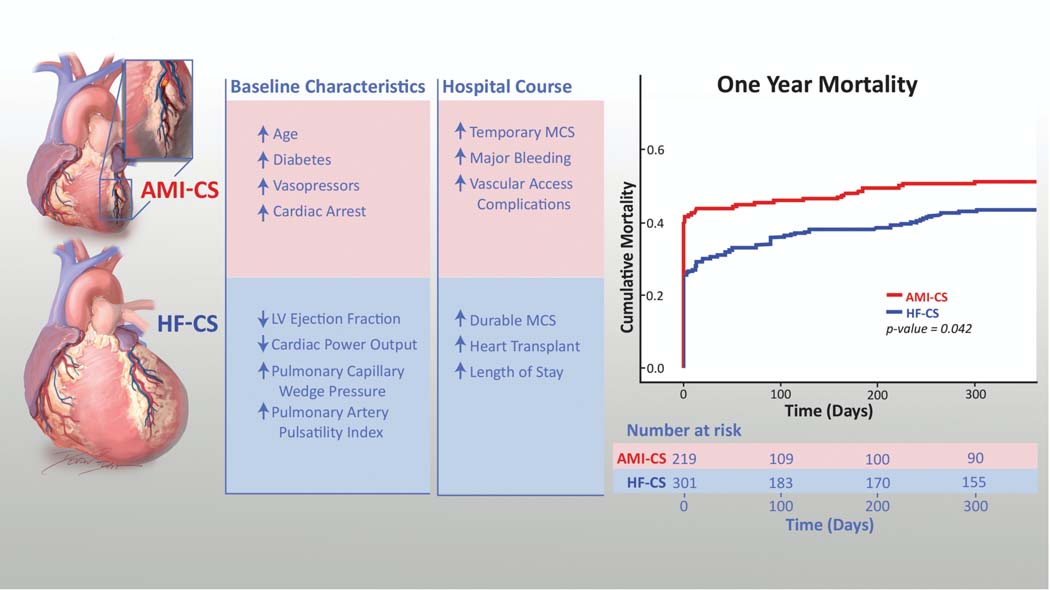
Results: Mean age was 61.5±13.5 years, 71% were male, 22% were Black patients, and 63% had chronic kidney disease. The HF-CS cohort was younger (58.5 versus 65.6 years, P<0.001), had fewer cardiac arrests (15.9% versus 35.2%, P<0.001), less vasopressor utilization (61.8% versus 82.2%, P<0.001), higher pulmonary artery pulsatility index (2.14 versus 1.51, P<0.01), lower cardiac power output (0.64 versus 0.77 W, P<0.01) and higher pulmonary capillary wedge pressure (25.4 versus 22.2 mm Hg, P<0.001) than patients with AMI-CS. Patients with HF-CS received less temporary mechanical circulatory support (34.9% versus 76.3% P<0.001) and experienced lower rates of major bleeding (17.3% versus 26.0%, P=0.02) and in-hospital mortality (23.9% versus 39.3%, P<0.001). Postdischarge, 133 AMI-CS and 229 patients with HF-CS experienced similar rates of 30-day readmission (19.5% versus 24.5%, P=0.30) and major adverse cardiac and cerebrovascular events (23.3% versus 28.8%, P=0.45). Patients with HF-CS had lower 1-year mortality (n=123, 42.6%) compared to the patients with AMI-CS (n=110, 52.9%, P=0.03). Cumulative 1-year mortality was also lower in patients with HF-CS (log-rank test, P=0.04).
Conclusions: Patients with HF-CS were younger, and despite lower cardiac power output and higher pulmonary capillary wedge pressure, less likely to receive vasopressors or temporary mechanical circulatory support. Although patients with HF-CS had lower in-hospital and 1-year mortality, both cohorts experienced similarly high rates of postdischarge major adverse cardiovascular and cerebrovascular events and 30-day readmission, highlighting that both cohorts warrant careful long-term follow-up.
Registration: URL: https://www.
Clinicaltrials: gov; Unique identifier: NCT03378739.
Keywords: heart failure; hemodynamics; mortality; myocardial infarction; shock, cardiogenic.
Figures
References
-
- Sv Diepen, Katz JN, Albert NM, Henry TD, Jacobs AK, Kapur NK, Kilic A, Menon V, Ohman EM, Sweitzer NK, et al. Contemporary Management of Cardiogenic Shock: A Scientific Statement From the American Heart Association. Circulation. 2017;136:e232–e268. - PubMed
-
- Thiele H, Ohman EM, de Waha-Thiele S, Zeymer U and Desch S. Management of cardiogenic shock complicating myocardial infarction: an update 2019. Eur Heart J. 2019;40:2671–2683. - PubMed
-
- Damluji AA, Bandeen-Roche K, Berkower C, Boyd CM, Al-Damluji MS, Cohen MG, Forman DE, Chaudhary R, Gerstenblith G, Walston JD, Ret al. Percutaneous Coronary Intervention in Older Patients With ST-Segment Elevation Myocardial Infarction and Cardiogenic Shock. J Am Coll Cardiol. 2019;73:1890–1900. - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
