

Evaluating Distance Bias in Chronic Rhinosinusitis Outcomes
- PMID: 35511170
- PMCID: PMC9073660
- DOI: 10.1001/jamaoto.2022.0268
Evaluating Distance Bias in Chronic Rhinosinusitis Outcomes
Abstract
Importance: The distance traveled by patients for medical care is associated with patient outcomes (ie, distance bias) and is a limitation in outcomes research. However, to date, distance bias has not been examined in rhinologic studies.
Objective: To evaluate the association of distance traveled by a cohort of patients with chronic rhinosinusitis with baseline disease severity and treatment outcomes.
Design, setting, and participants: A total of 505 patients with chronic rhinosinusitis were prospectively enrolled in a multi-institutional, cross-sectional study in academic tertiary care centers between April 2011 and January 2020. Participants self-selected continued appropriate medical therapy or endoscopic sinus surgery. The 22-item Sinonasal Outcome Test (SNOT-22) and Medical Outcomes Study Short Form 6-D (SF-6D) health utility value scores were recorded at enrollment and follow-up. Data on the distances traveled by patients to the medical centers, based on residence zip codes, and medical comorbid conditions were collected.
Exposures: Distance traveled by patient to obtain rhinologic care.
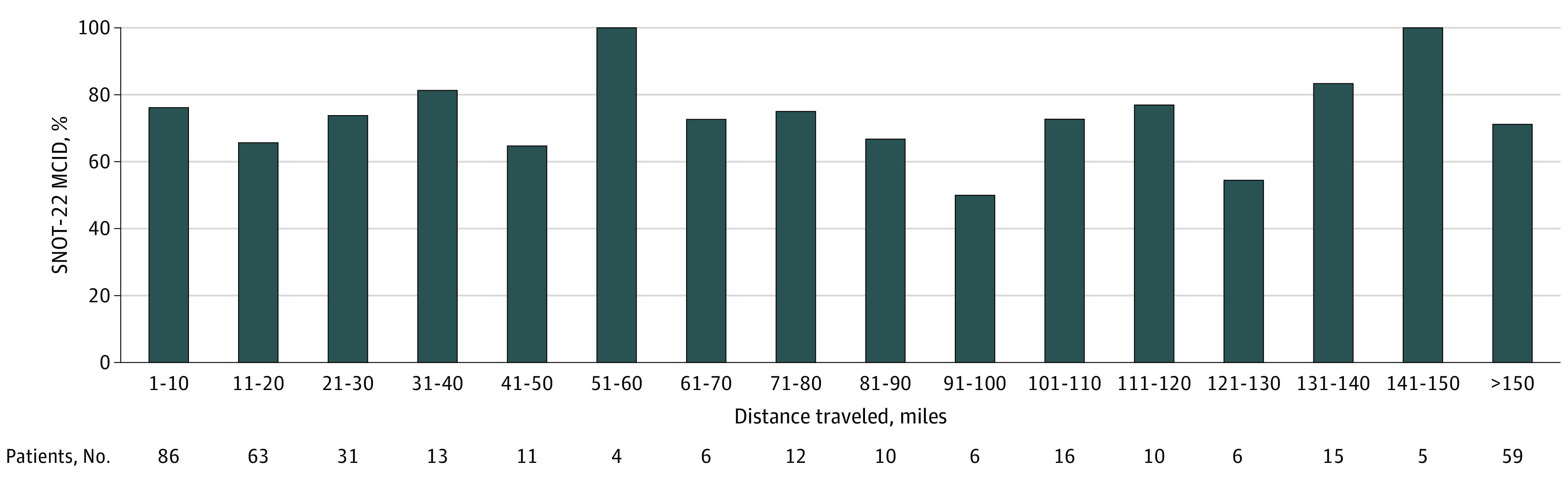
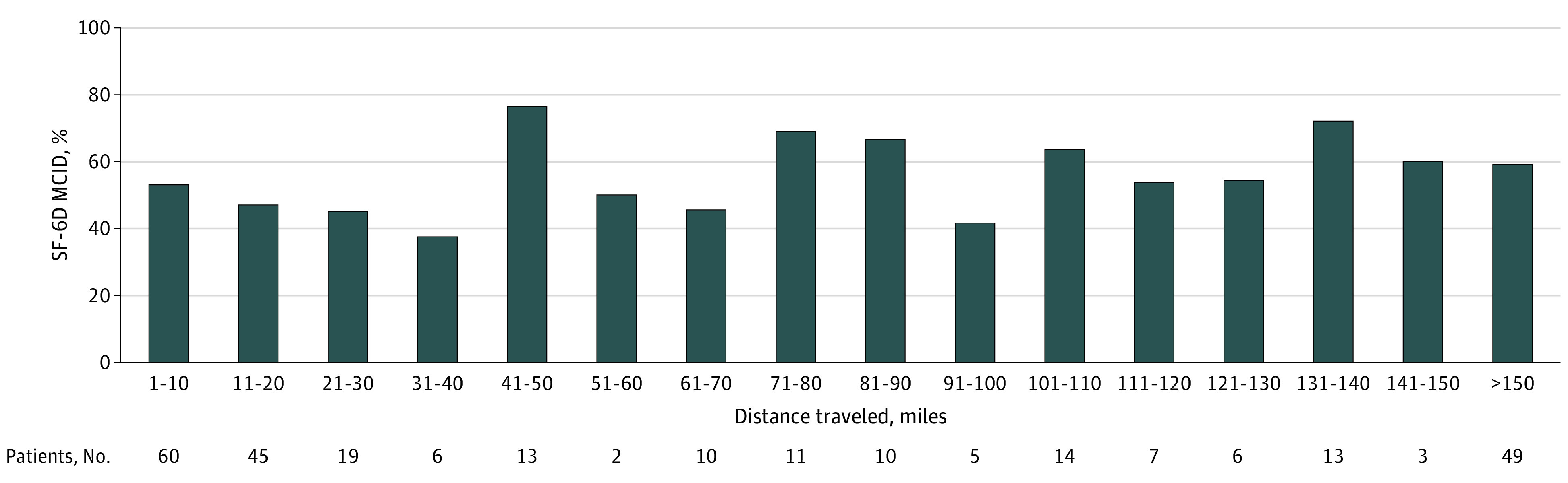
Main outcomes and measures: SNOT-22 and SF-6D scores. Scores for SNOT-22 range from 0 to 110; and for SF-6D, from 0.0 to 1.0. Higher SNOT-22 total scores indicate worse overall symptom severity. Higher SF-6D scores indicate better overall health utility; 1.0 represents perfect health and 0.0 represents death.
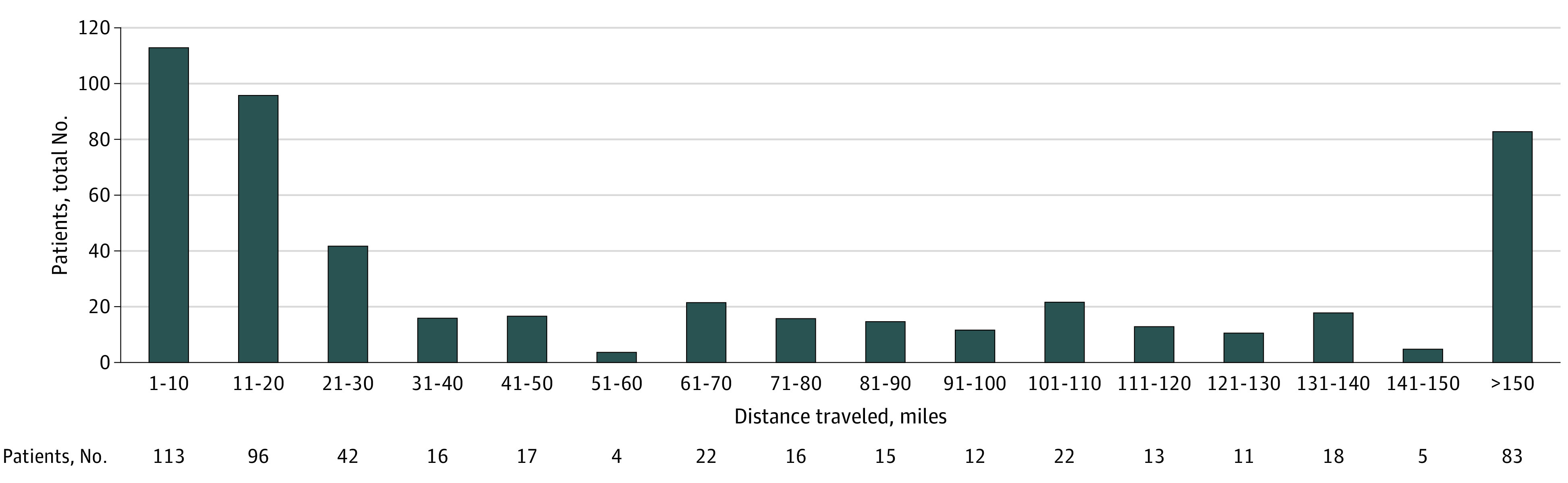
Results: The median age for the 505 participants was 56.0 years (IQR, 41.0-64.0 years), 261 were men (51.7%), 457 were White (90.5%), and 13 were Hispanic or Latino (2.6%). These categories were collected according to criteria described and required by the National Institutes of Health and therefore do not equal the entire cohort. Patients traveled a median distance of 31.6 miles (50.6 km) (IQR, 12.2-114.5 miles [19.5-183.2 km]). Baseline (r = 0.00; 95% CI, 0.00-0.18) and posttreatment (r = 0.01; 95% CI, -0.07 to 0.10) SNOT-22 scores, as well as baseline (r = -0.12; 95% CI, -0.21 to -0.04) and posttreatment (r = 0.07; 95% CI, -0.02 to 0.16) SF-6D scores, were not associated with distance. There was no clinically meaningful correlation between distance traveled and mean comorbidity burden. Nevertheless, patients with a history of endoscopic sinus surgery were more likely to travel longer distances to obtain care (Cliff delta = 0.28; 95% CI, 0.19-0.38).
Conclusions and relevance: Although this cross-sectional study found that some patients appear more willing to travel longer distances for chronic rhinosinusitis care, results suggest that distance traveled to academic tertiary care centers was not associated with disease severity, outcomes, or comorbidity burden. These findings argue for greater generalizability of study results across various cohorts independent of distance traveled to obtain rhinologic care.
Trial registration: ClinicalTrials.gov Identifier: NCT02720653.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
