

Pediatric metanephric adenoma with Fanconi-Bickel syndrome: a case report and review of literature
- PMID: 35511306
- PMCID: PMC9072611
- DOI: 10.1186/s40792-022-01435-4
Pediatric metanephric adenoma with Fanconi-Bickel syndrome: a case report and review of literature
Abstract
Background: Metanephric adenoma (MA) is a rare benign renal tumor that resembles renal cell carcinoma and Wilms' tumor in radiological as well as pathological appearance. It can present at any age or gender, and it is extremely rare in the pediatric age group with less than 50 reported cases. Fanconi-Bickel syndrome (FBS) is a rare autosomal recessive disorder of carbohydrate metabolism. Herein, we report a rare incidence of MA in a boy with a genetically confirmed FBS who underwent a nephron-sparing surgery.
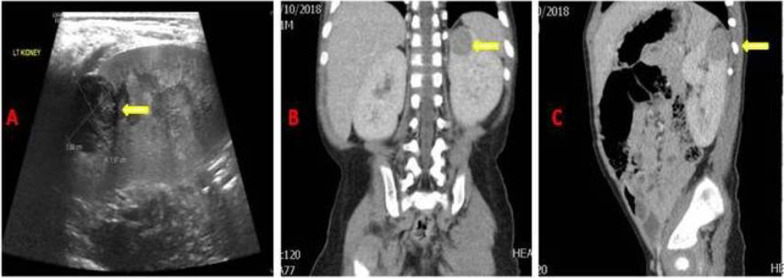
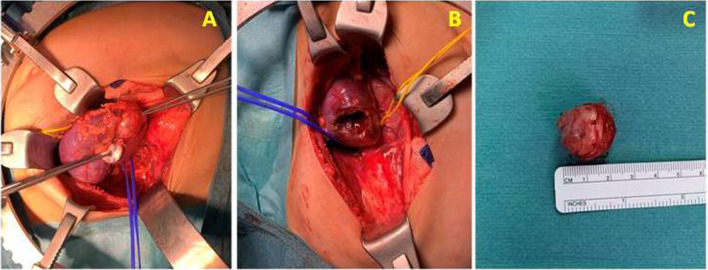
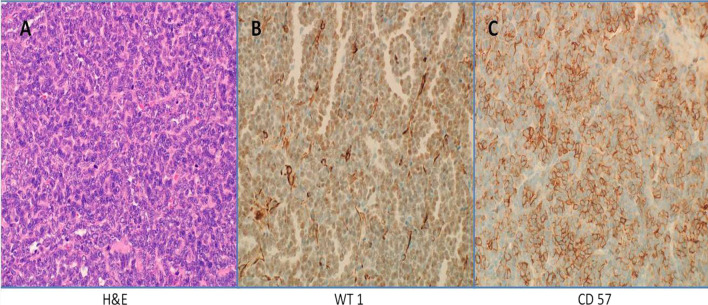
Case presentation: A 21-month-old boy was referred to the pediatric urology clinic for further evaluation of an incidentally discovered left renal mass. His laboratory investigations showed normal renal function, hypophosphatemia, high blood glucose level, markedly elevated serum alkaline phosphatase, and low serum vitamin D. Blood picture showed signs of polycythemia and urinalysis showed glucosuria and aminoaciduria. Genetic testing was positive for Fanconi-Bickel syndrome. Radiological investigations were carried out with abdominal ultrasound and computerized tomography (CT) with intravenous contrast documented a sharply marginated peripheral hypoechoic hypovascular homogeneously enhancing mass at the upper pole of the left kidney measuring 2.0 × 1.8 × 2.0 cm. The child was admitted and started on supportive treatment until his medical condition was stabilized, then underwent elective open left partial nephrectomy via a left upper transverse abdominal transperitoneal incision. The excised renal mass was sent for histopathological assessment and was found to be a tumor composed of tightly packed tubules with no mitotic figures or necrosis and scanty cytoplasm consistent with MA. After good hydration and tumor resection, his polycythemia gradually improved. The patient was discharged home in a good condition with his proper replacement therapies. His follow-up abdominal ultrasound after 12 months showed no signs of recurrence.
Conclusions: Metanephric adenoma is extremely rare in the pediatric age group, especially in those who have a FBS. The only way to diagnose and treat this tumor is by surgical resection as most patients are asymptomatic. A nephron-sparing surgery is better for this age group in which the future renal function is considered.
Keywords: Fanconi–Bickel syndrome; Metanephric adenoma; Nephrectomy; Outcome; Pediatric; Renal mass.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Metanephric adenoma in a pediatric patient case report.Front Pediatr. 2025 Apr 3;13:1539220. doi: 10.3389/fped.2025.1539220. eCollection 2025. Front Pediatr. 2025. PMID: 40248024 Free PMC article.
-
Metanephric Adenoma in the Pediatric Population: Diagnostic Challenges and Follow-up.Urology. 2018 Oct;120:211-215. doi: 10.1016/j.urology.2018.06.042. Epub 2018 Jul 10. Urology. 2018. PMID: 30006267 Review.
-
Metanephric adenoma diagnosed on biopsy in an infant: a case report.J Med Case Rep. 2023 Aug 8;17(1):354. doi: 10.1186/s13256-023-04046-1. J Med Case Rep. 2023. PMID: 37550779 Free PMC article.
-
Metanephric adenoma treated with laparoscopic nephrectomy: A case report.Mol Clin Oncol. 2017 Sep;7(3):404-406. doi: 10.3892/mco.2017.1327. Epub 2017 Jul 18. Mol Clin Oncol. 2017. PMID: 28894579 Free PMC article.
-
Metanephric adenoma in an 8-year-old child: case report and review of the literature.J Pediatr Surg. 2005 May;40(5):e25-8. doi: 10.1016/j.jpedsurg.2005.02.019. J Pediatr Surg. 2005. PMID: 15937802 Review.
Cited by
-
Effects of antibiotic exposure on risks of colorectal tumors: a systematic review and meta-analysis.J Transl Med. 2025 Jun 18;23(1):682. doi: 10.1186/s12967-025-06727-5. J Transl Med. 2025. PMID: 40533779 Free PMC article. Review.
-
Metanephric adenoma in children: A case report and literature review.Oncol Lett. 2023 Sep 27;26(5):486. doi: 10.3892/ol.2023.14073. eCollection 2023 Nov. Oncol Lett. 2023. PMID: 37818137 Free PMC article.
-
Metanephric adenoma in a pediatric patient case report.Front Pediatr. 2025 Apr 3;13:1539220. doi: 10.3389/fped.2025.1539220. eCollection 2025. Front Pediatr. 2025. PMID: 40248024 Free PMC article.
-
Clinical, genetic profile and therapy evaluation of 11 Chinese pediatric patients with Fanconi-Bickel syndrome.Orphanet J Rare Dis. 2024 Feb 16;19(1):75. doi: 10.1186/s13023-024-03070-8. Orphanet J Rare Dis. 2024. PMID: 38365697 Free PMC article.
References
LinkOut - more resources
Full Text Sources
