

The Kenevo microprocessor-controlled prosthetic knee compared with non-microprocessor-controlled knees in individuals older than 65 years in Sweden: A cost-effectiveness and budget-impact analysis
- PMID: 35511441
- PMCID: PMC9554759
- DOI: 10.1097/PXR.0000000000000138
The Kenevo microprocessor-controlled prosthetic knee compared with non-microprocessor-controlled knees in individuals older than 65 years in Sweden: A cost-effectiveness and budget-impact analysis
Abstract
Background: Growing evidence suggests that individuals with transfemoral amputation or knee disarticulation using a prosthesis equipped with a microprocessor-controlled knee (MPK) benefit from enhanced mobility and safety, including less falls. In elderly individuals, high mortality rates are assumed to reduce the expected useful life of MPKs, and this raises concerns regarding their economic effectiveness.
Objective: To investigate the cost-effectiveness and budget impact of the Kenevo/MPK (Ottobock, Germany) compared with non-microprocessor-controlled knees (NMPKs) in people older than 65 years at the time of transfemoral amputation/knee disarticulation, from a Swedish payer's perspective.
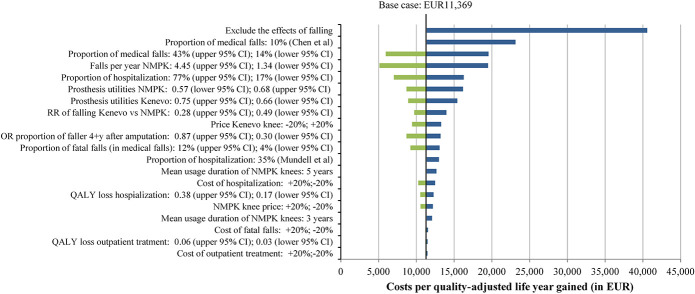
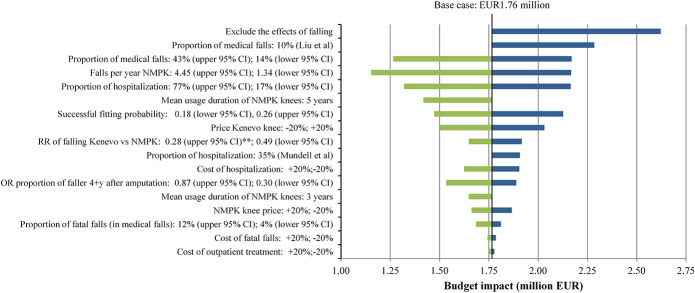
Methods: A decision-analytic model was developed to conduct the economic analysis of the Kenevo/MPK. Model parameters were derived from Swedish databases and published literature. Univariate and probabilistic sensitivity analyses were performed to explore parameter uncertainty.
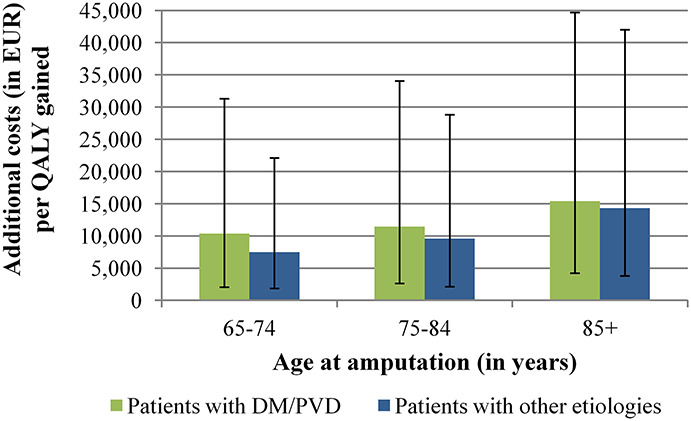
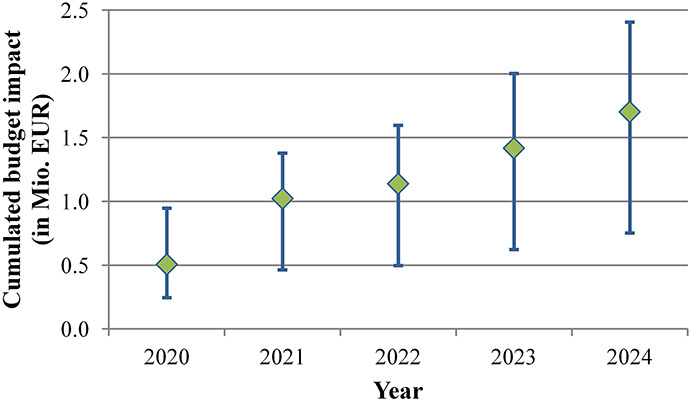
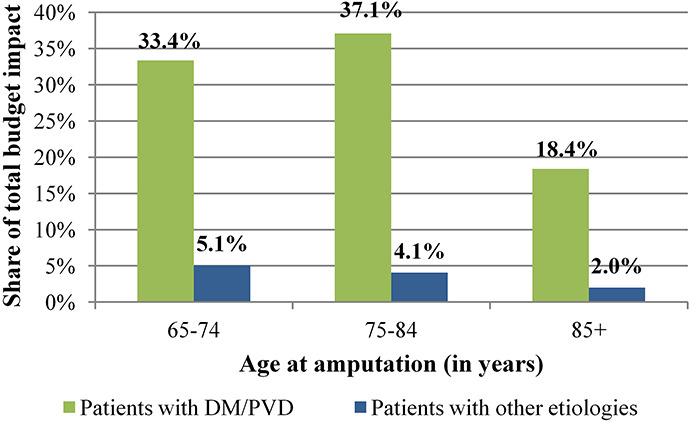
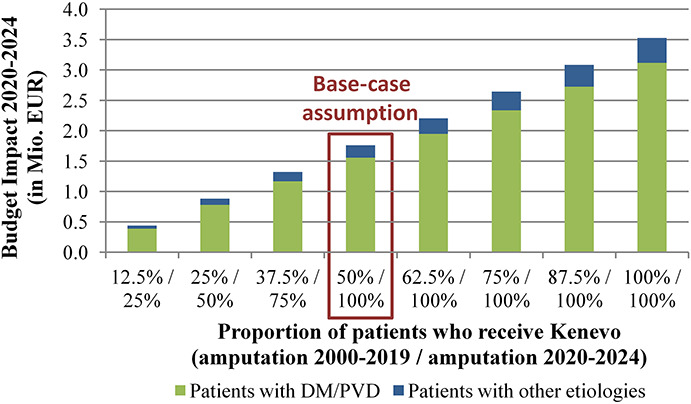
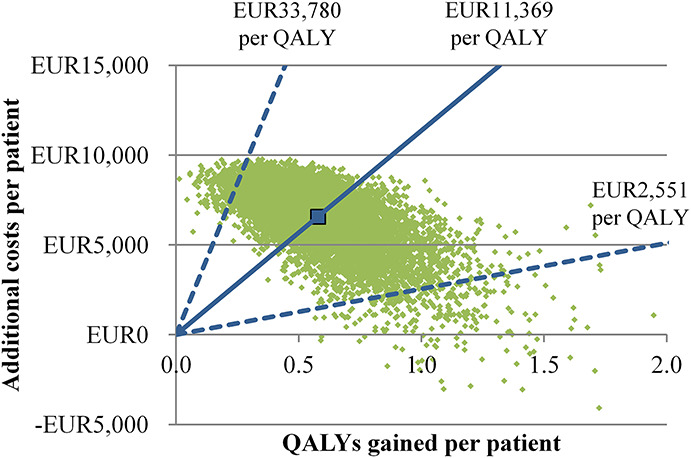
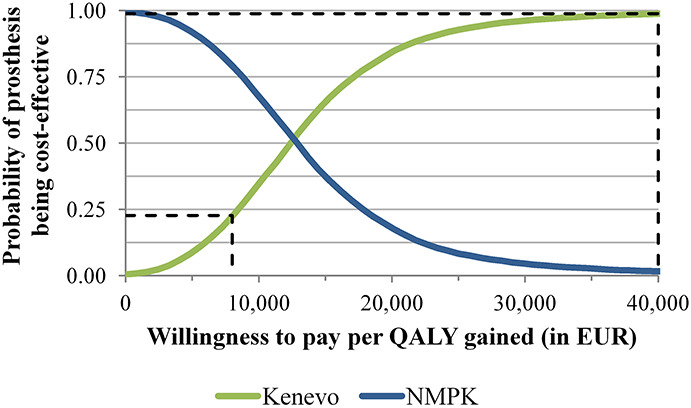
Results: Compared with NMPKs, the Kenevo/MPK reduced the frequency of hospitalizations by 137 per 1,000 person years while the frequency of fatal falls was reduced by 19 per 1,000 person-years in the simulation. Over a 25-year time horizon, the incremental cost-effectiveness ratio was EUR11,369 per quality-adjusted life year. The probability of the MPK being cost-effective at a threshold of EUR40,000 per quality-adjusted life year was 99%. The 5-year budget impact model predicted an increase in payer expenditure of EUR1.76 million if all new patients received a Kenevo/MPK, and 50% of current NMPK users switched to the MPK.
Conclusions: Results of the modeling suggest that the Kenevo/MPK is likely to be cost-effective for elderly individuals, primarily because of a reduction in falls.
Copyright © 2022 The Authors. Published by Wolters Kluwer incorporated on behalf of The International Society for Prosthetics and Orthotics.
Figures

Similar articles
-
Cost-effectiveness and budget impact of the microprocessor-controlled knee C-Leg in transfemoral amputees with and without diabetes mellitus.Eur J Health Econ. 2020 Apr;21(3):437-449. doi: 10.1007/s10198-019-01138-y. Epub 2020 Jan 2. Eur J Health Econ. 2020. PMID: 31897813 Free PMC article.
-
Economic benefits of microprocessor controlled prosthetic knees: a modeling study.J Neuroeng Rehabil. 2018 Sep 5;15(Suppl 1):62. doi: 10.1186/s12984-018-0405-8. J Neuroeng Rehabil. 2018. PMID: 30255802 Free PMC article. Review.
-
Mobility and satisfaction with a microprocessor-controlled knee in moderately active amputees: A multi-centric randomized crossover trial.Ann Phys Rehabil Med. 2018 Sep;61(5):278-285. doi: 10.1016/j.rehab.2018.04.003. Epub 2018 May 16. Ann Phys Rehabil Med. 2018. PMID: 29753888 Clinical Trial.
-
Safety and function of a prototype microprocessor-controlled knee prosthesis for low active transfemoral amputees switching from a mechanic knee prosthesis: a pilot study.Disabil Rehabil Assist Technol. 2018 Feb;13(2):157-165. doi: 10.1080/17483107.2017.1300344. Epub 2017 Apr 11. Disabil Rehabil Assist Technol. 2018. PMID: 28399722 Clinical Trial.
-
Benefits of the Genium microprocessor controlled prosthetic knee on ambulation, mobility, activities of daily living and quality of life: a systematic literature review.Disabil Rehabil Assist Technol. 2021 Jul;16(5):453-464. doi: 10.1080/17483107.2019.1648570. Epub 2019 Aug 30. Disabil Rehabil Assist Technol. 2021. PMID: 31469023
References
-
- Sansam K, Neumann V, O'Connor R, et al. . Predicting walking ability following lower limb amputation: a systematic review of the literature. J Rehabil Med 2009; 41: 593–603. - PubMed
-
- Torbjörnsson E, Blomgren L, Fagerdahl AM, et al. . Risk factors for amputation are influenced by competing risk of death in patients with critical limb ischemia. J Vasc Surg 2020; 71: 130. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
