

HIP1R and vimentin immunohistochemistry predict 1p/19q status in IDH-mutant glioma
- PMID: 35511748
- PMCID: PMC9713528
- DOI: 10.1093/neuonc/noac111
HIP1R and vimentin immunohistochemistry predict 1p/19q status in IDH-mutant glioma
Abstract
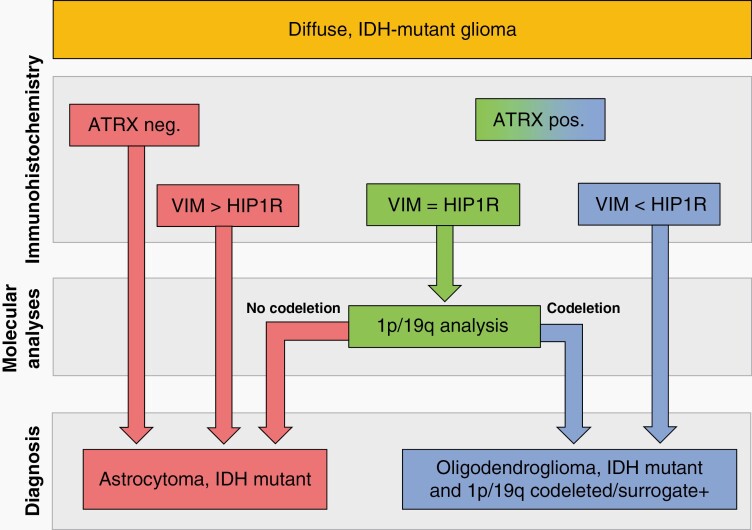
Background: IDH-mutant gliomas are separate based on the codeletion of the chromosomal arms 1p and 19q into oligodendrogliomas IDH-mutant 1p/19q-codeleted and astrocytomas IDH-mutant. While nuclear loss of ATRX expression excludes 1p/19q codeletion, its limited sensitivity prohibits to conclude on 1p/19q status in tumors with retained nuclear ATRX expression.
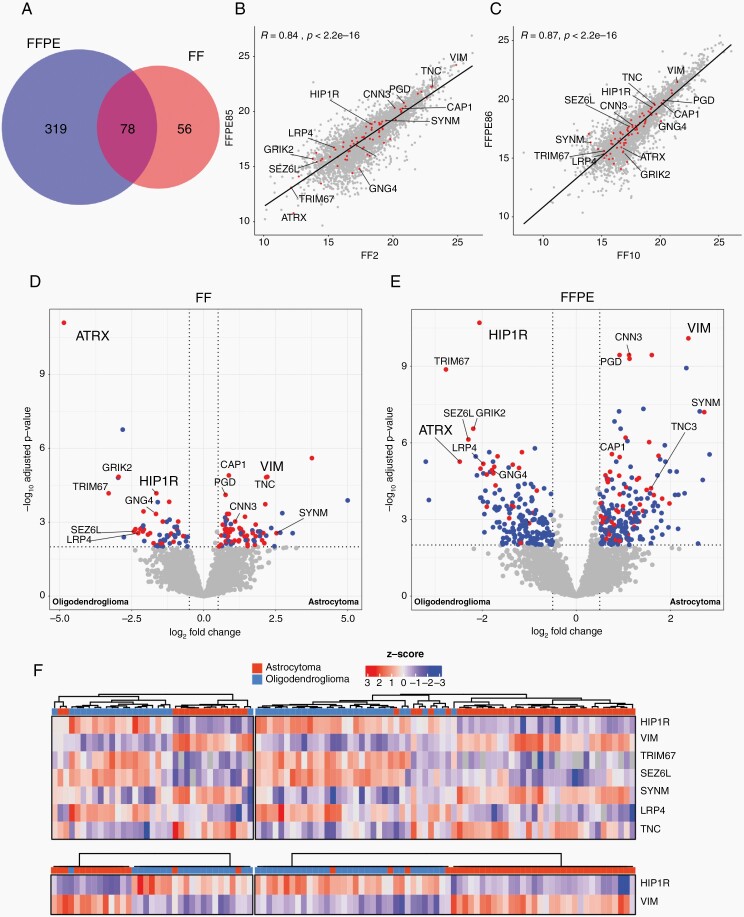
Methods: Employing mass spectrometry based proteomic analysis in a discovery series containing 35 fresh frozen and 72 formalin fixed and paraffin embedded tumors with established IDH and 1p/19q status, potential biomarkers were discovered. Subsequent validation immunohistochemistry was conducted on two independent series (together 77 oligodendrogliomas IDH-mutant 1p/19q-codeleted and 92 astrocytomas IDH-mutant).
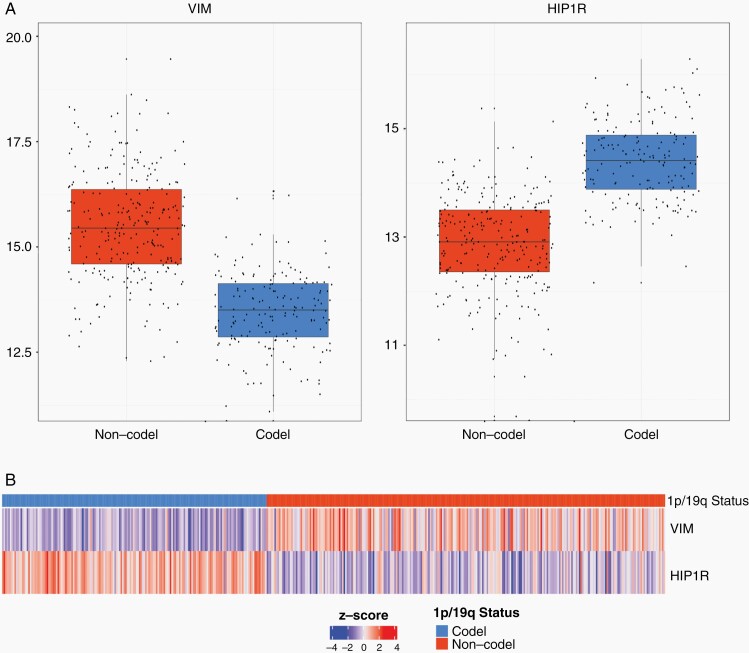
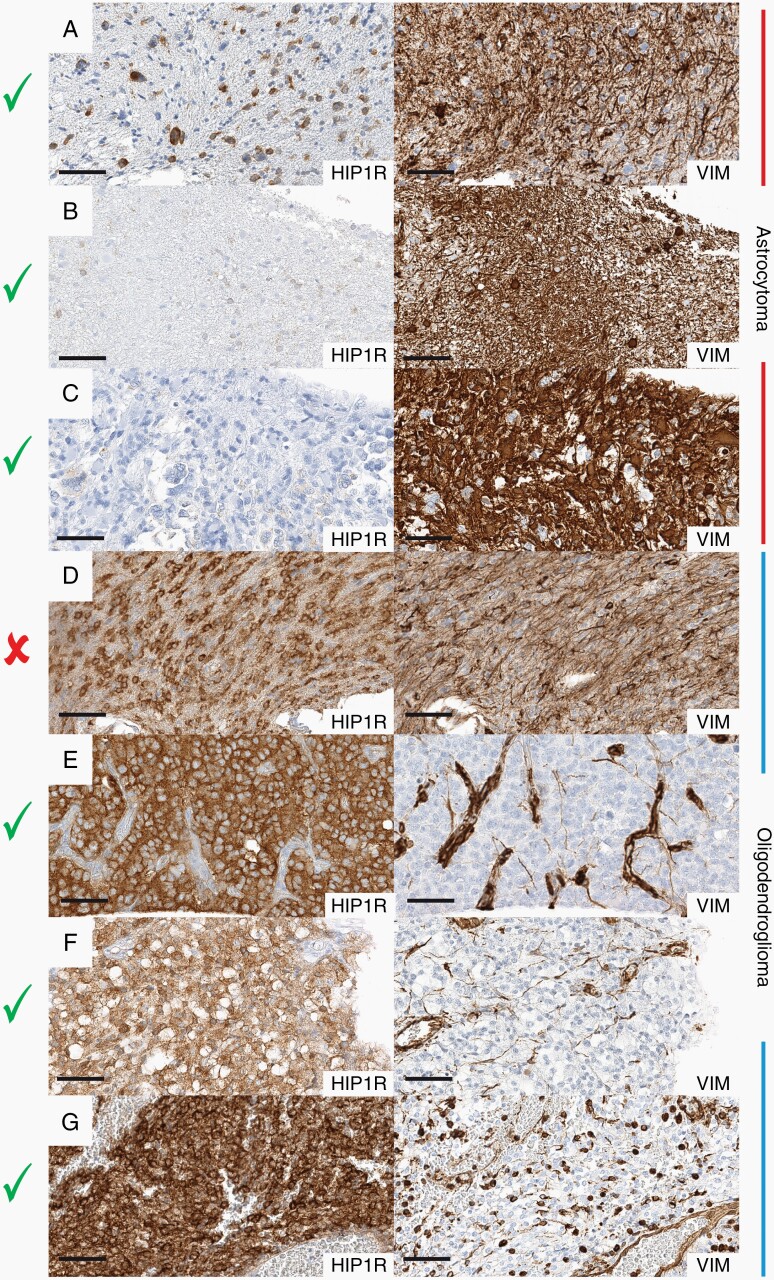
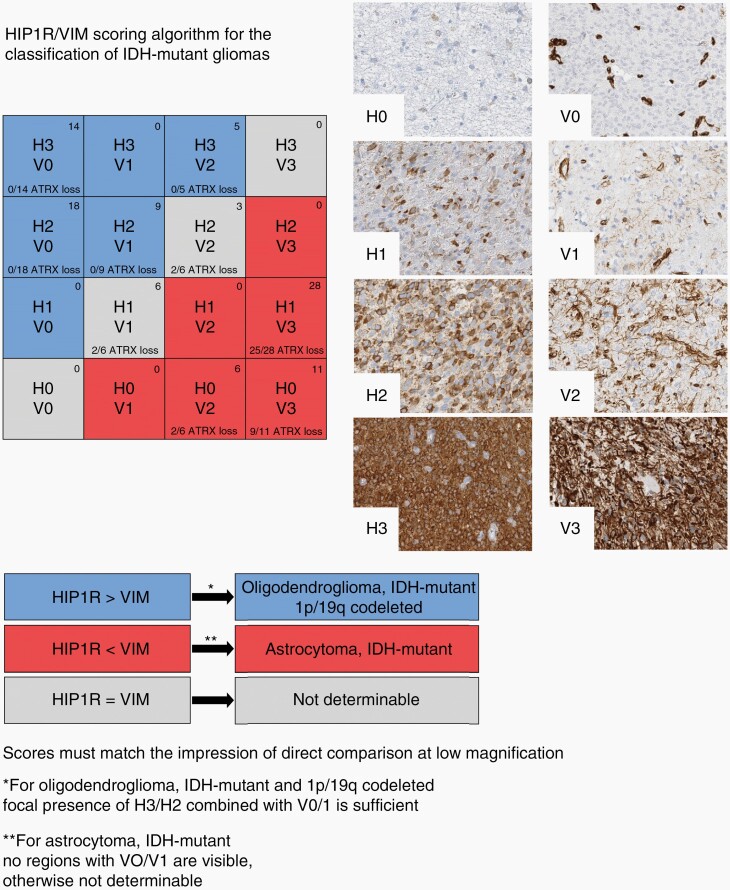
Results: We detected highly specific protein patterns distinguishing oligodendroglioma and astrocytoma. In these patterns, high HIP1R and low vimentin levels were observed in oligodendroglioma while low HIP1R and high vimentin levels occurred in astrocytoma. Immunohistochemistry for HIP1R and vimentin expression in 35 cases from the FFPE discovery series confirmed these findings. Blinded evaluation of the validation cohorts predicted the 1p/19q status with a positive and negative predictive value as well as an accuracy of 100% in the first cohort and with a positive predictive value of 83%; negative predictive value of 100% and an accuracy of 92% in the second cohort. Nuclear ATRX loss as marker for astrocytoma increased the sensitivity to 96% and the specificity to 100%.
Conclusions: We demonstrate that immunohistochemistry for HIP1R, vimentin, and ATRX predict 1p/19q status with 100% specificity and 95% sensitivity and therefore, constitutes a simple and inexpensive approach to the classification of IDH-mutant glioma.
Keywords: 1p/19q; ATRX; HIP1R; IDH; Vimentin; proteomics.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Louis DN, Ohgaki H, Wiestler OD, et al. . WHO Classification and Grading of Tumours of the Central Nervous System. Lyon: IARC Press; International Agency for Research on Cancer; 2016.
-
- Balss J, Meyer J, Mueller W, et al. . Analysis of the IDH1 codon 132 mutation in brain tumors. Acta Neuropathol. 2008; 116(6):597–602. - PubMed
-
- Capper D, Zentgraf H, Balss J, Hartmann C, von Deimling A. Monoclonal antibody specific for IDH1 R132H mutation. Acta Neuropathol. 2009; 118(5):599–601. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
