

Left ventricular remodelling post-myocardial infarction: pathophysiology, imaging, and novel therapies
- PMID: 35511857
- PMCID: PMC9336586
- DOI: 10.1093/eurheartj/ehac223
Left ventricular remodelling post-myocardial infarction: pathophysiology, imaging, and novel therapies
Abstract
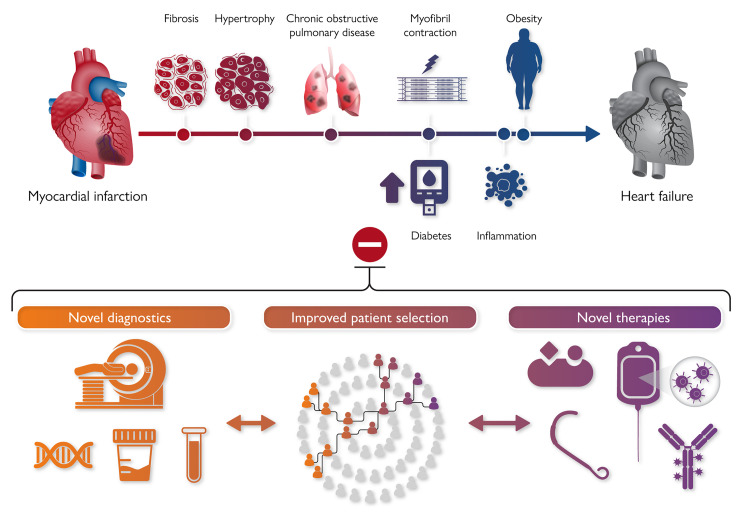
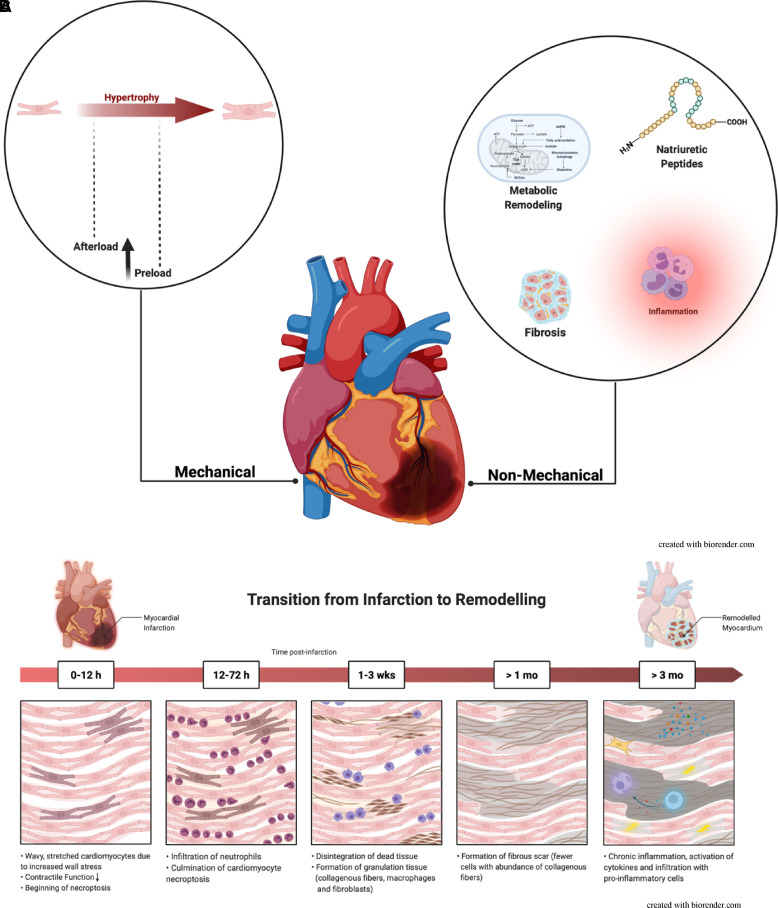
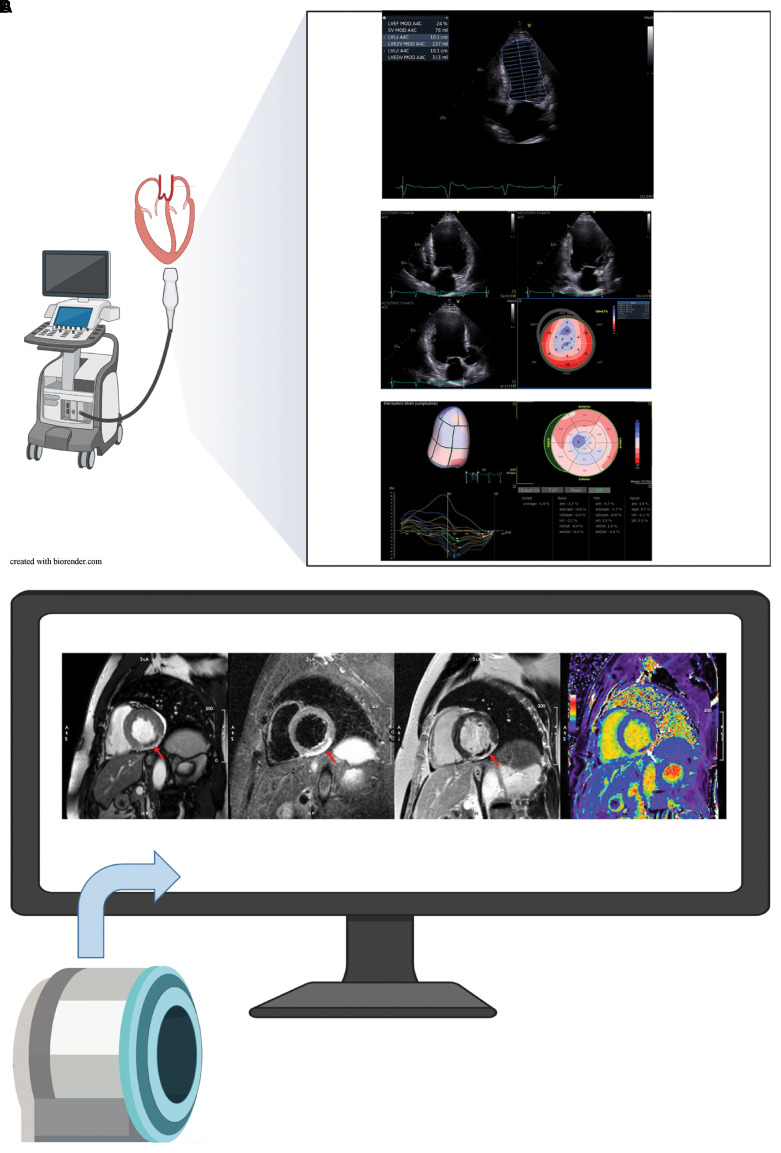
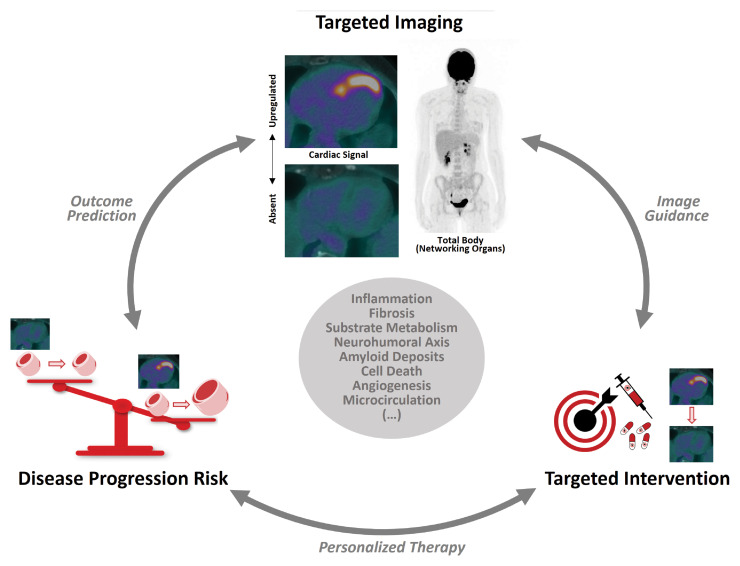
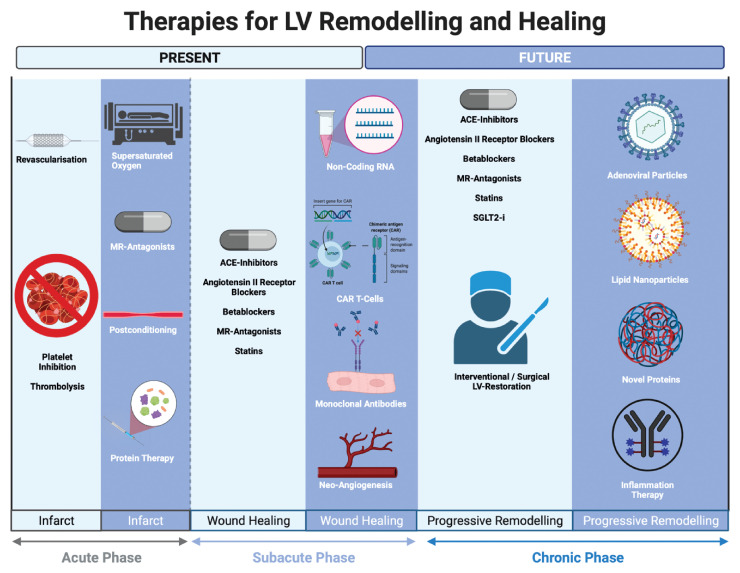
Most patients survive acute myocardial infarction (MI). Yet this encouraging development has certain drawbacks: heart failure (HF) prevalence is increasing and patients affected tend to have more comorbidities worsening economic strain on healthcare systems and impeding effective medical management. The heart's pathological changes in structure and/or function, termed myocardial remodelling, significantly impact on patient outcomes. Risk factors like diabetes, chronic obstructive pulmonary disease, female sex, and others distinctly shape disease progression on the 'road to HF'. Despite the availability of HF drugs that interact with general pathways involved in myocardial remodelling, targeted drugs remain absent, and patient risk stratification is poor. Hence, in this review, we highlight the pathophysiological basis, current diagnostic methods and available treatments for cardiac remodelling following MI. We further aim to provide a roadmap for developing improved risk stratification and novel medical and interventional therapies.
Keywords: Fibrosis; Heart failure; Myocardial Infarction; Remodelling.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Cardiology.
Figures
References
-
- Bolognese L, Neskovic AN, Parodi G, Cerisano G, Buonamici P, Santoro GM, et al. Left ventricular remodeling after primary coronary angioplasty: patterns of left ventricular dilation and long-term prognostic implications. Circulation 2002;106:2351–2357. - PubMed
-
- Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, et al. Heart disease and stroke statistics-2020 update: a report from the American Heart Association. Circulation 2020;141:e139–e596. - PubMed
-
- Stork S, Hense HW, Zentgraf C, Uebelacker I, Jahns R, Ertl G, et al. Pharmacotherapy according to treatment guidelines is associated with lower mortality in a community-based sample of patients with chronic heart failure: a prospective cohort study. Eur J Heart Fail 2008;10:1236–1245. - PubMed
-
- Desta L, Jernberg T, Spaak J, Hofman-Bang C, Persson H. Risk and predictors of readmission for heart failure following a myocardial infarction between 2004 and 2013: a Swedish nationwide observational study. Int J Cardiol 2017;248:221–226. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
