

Cardiac magnetic resonance identifies raised left ventricular filling pressure: prognostic implications
- PMID: 35512290
- PMCID: PMC9259376
- DOI: 10.1093/eurheartj/ehac207
Cardiac magnetic resonance identifies raised left ventricular filling pressure: prognostic implications
Abstract
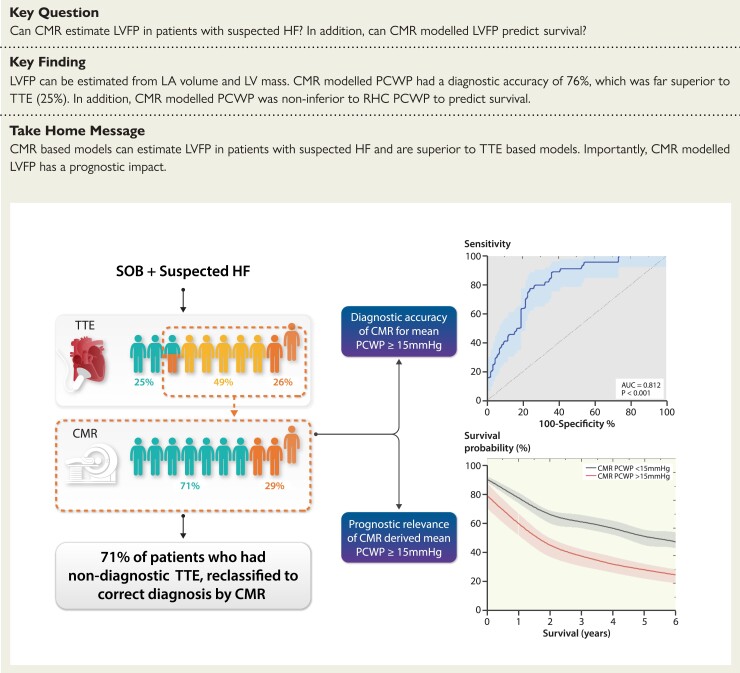
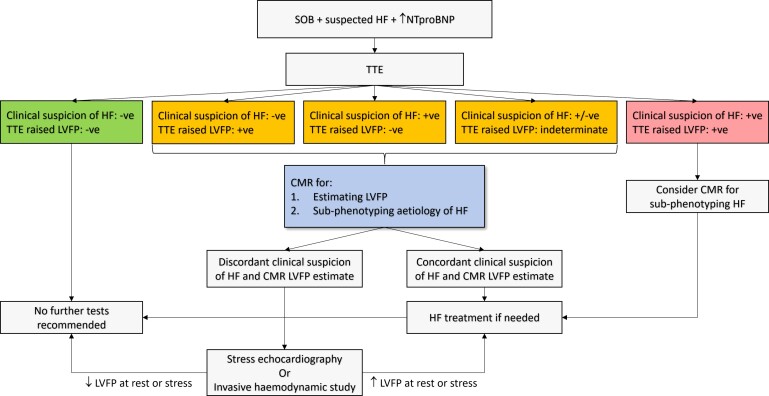
Aims: Non-invasive imaging is routinely used to estimate left ventricular (LV) filling pressure (LVFP) in heart failure (HF). Cardiovascular magnetic resonance (CMR) is emerging as an important imaging tool for sub-phenotyping HF. However, currently, LVFP cannot be estimated from CMR. This study sought to investigate (i) if CMR can estimate LVFP in patients with suspected HF and (ii) if CMR-modelled LVFP has prognostic power.
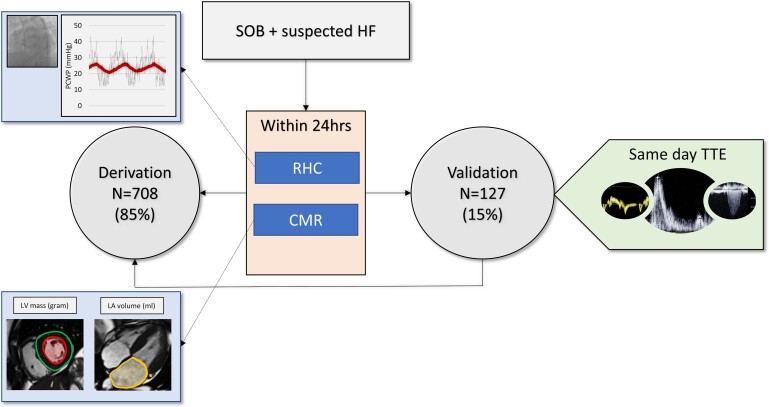
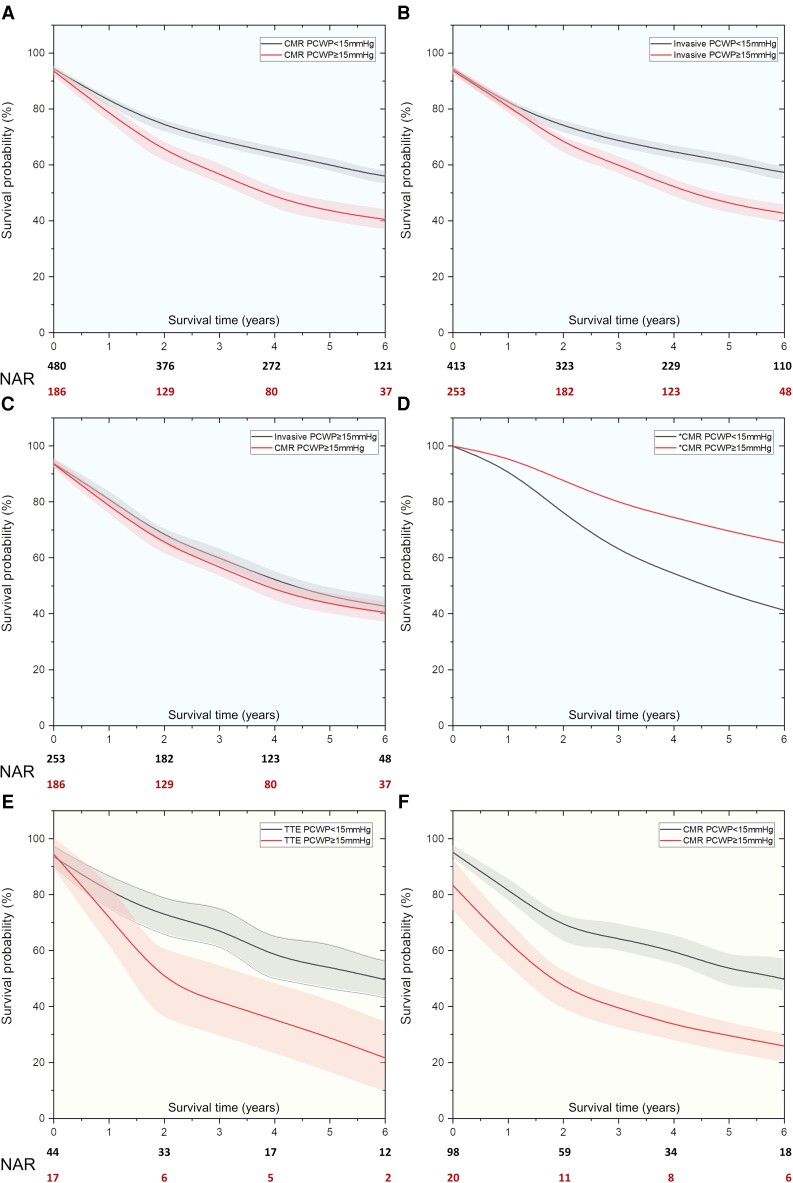
Methods and results: Suspected HF patients underwent right heart catheterization (RHC), CMR and transthoracic echocardiography (TTE) (validation cohort only) within 24 h of each other. Right heart catheterization measured pulmonary capillary wedge pressure (PCWP) was used as a reference for LVFP. At follow-up, death was considered as the primary endpoint. We enrolled 835 patients (mean age: 65 ± 13 years, 40% male). In the derivation cohort (n = 708, 85%), two CMR metrics were associated with RHC PCWP:LV mass and left atrial volume. When applied to the validation cohort (n = 127, 15%), the correlation coefficient between RHC PCWP and CMR-modelled PCWP was 0.55 (95% confidence interval: 0.41-0.66, P < 0.0001). Cardiovascular magnetic resonance-modelled PCWP was superior to TTE in classifying patients as normal or raised filling pressures (76 vs. 25%). Cardiovascular magnetic resonance-modelled PCWP was associated with an increased risk of death (hazard ratio: 1.77, P < 0.001). At Kaplan-Meier analysis, CMR-modelled PCWP was comparable to RHC PCWP (≥15 mmHg) to predict survival at 7-year follow-up (35 vs. 37%, χ2 = 0.41, P = 0.52).
Conclusion: A physiological CMR model can estimate LVFP in patients with suspected HF. In addition, CMR-modelled LVFP has a prognostic role.
Keywords: Cardiovascular magnetic resonance; Left ventricular filling pressure; Right heart catheterization.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Cardiovascular magnetic resonance for the assessment of left ventricular filling pressure in heart failure.Eur Heart J. 2022 Jul 7;43(26):2523-2525. doi: 10.1093/eurheartj/ehac247. Eur Heart J. 2022. PMID: 35574820 No abstract available.
-
Left atrial volume and left ventricular mass for pulmonary capillary wedge pressure assessment with cardiovascular magnetic resonance: accurate enough for clinical use?Eur Heart J. 2023 Feb 1;44(5):425-426. doi: 10.1093/eurheartj/ehac739. Eur Heart J. 2023. PMID: 36514969 No abstract available.
-
Cardiovascular magnetic resonance can improve the precision for left ventricular filling pressure assessment.Eur Heart J. 2023 Feb 1;44(5):427-428. doi: 10.1093/eurheartj/ehac740. Eur Heart J. 2023. PMID: 36515072 No abstract available.
References
-
- Ponikowski P, Voors AA, Anker SDet al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failureThe Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2016;37:2129–2200. - PubMed
-
- Luchsinger PC, Seipp HW, Patel DJ. Relationship of pulmonary artery-wedge pressure to left atrial pressure in man. Circ Res 1962;11:315–318. - PubMed
-
- Dorfs S, Zeh W, Hochholzer Wet al. Pulmonary capillary wedge pressure during exercise and long-term mortality in patients with suspected heart failure with preserved ejection fraction. Eur Heart J 2014;35:3103–3112. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
