

IDCRP Combat-Related Extremity Wound Infection Research
- PMID: 35512376
- PMCID: PMC9278329
- DOI: 10.1093/milmed/usab065
IDCRP Combat-Related Extremity Wound Infection Research
Abstract
Introduction: Extremity trauma is the most common battlefield injury, resulting in a high frequency of combat-related extremity wound infections (CEWIs). As these infections are associated with substantial morbidity and may impact wounded warriors long after initial hospitalization, CEWIs have been a focus of the Infectious Disease Clinical Research Program (IDCRP). Herein, we review findings of CEWI research conducted through the IDCRP and discuss future and ongoing analyses.
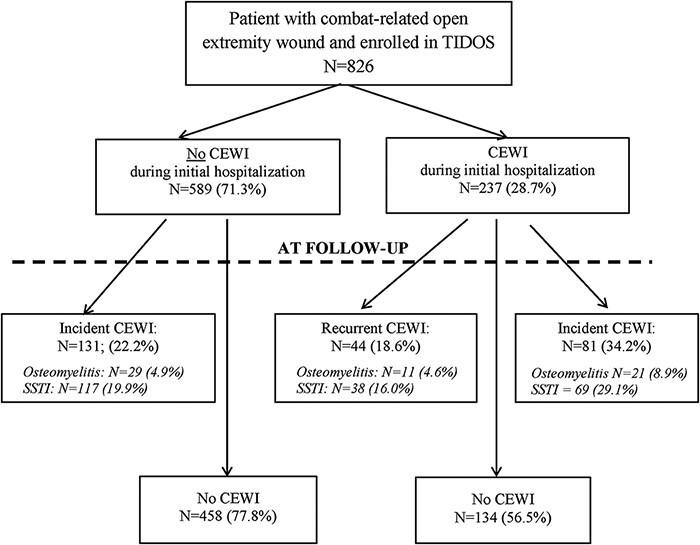
Methods: Military personnel with deployment-related trauma sustained between 2009 and 2014 were examined in retrospective analyses through the observational Trauma Infectious Disease Outcomes Study (TIDOS). Characteristics of wounded warriors with ≥1 open extremity wound were assessed, focusing on injury patterns and infection risk factors. Through a separate trauma-associated osteomyelitis study, military personnel with combat-related open fractures of the long bones (tibia, femur, and upper extremity) sustained between 2003 and 2009 were examined to identify osteomyelitis risk factors.
Results: Among 1,271 wounded warriors with ≥1 open extremity wound, 16% were diagnosed with a CEWI. When assessed by their most severe extremity injury (i.e., amputation, open fracture, or open soft-tissue wound), patients with amputations had the highest proportion of infections (47% of 212 patients with traumatic amputations). Factors related to injury pattern, mechanism, and severity were independent predictors of CEWIs during initial hospitalization. Having a non-extremity infection at least 4 days before CEWI diagnosis was associated with reduced likelihood of CEWI development. After hospital discharge, 28% of patients with extremity trauma had a new or recurrent CEWI during follow-up. Risk factors for the development of CEWIs during follow-up included injury pattern, having either a CEWI or other infection during initial hospitalization, and receipt of antipseudomonal penicillin for ≥7 days. A reduced likelihood for CEWIs during follow-up was associated with a hospitalization duration of 15-30 days. Under the retrospective osteomyelitis risk factor analysis, patients developing osteomyelitis had higher open fracture severity based on Gustilo-Anderson (GA) and the Orthopaedic Trauma Association classification schemes and more frequent traumatic amputations compared to open fracture patients without osteomyelitis. Recurrence of osteomyelitis was also common (28% of patients with open tibia fractures had a recurrent episode). Although osteomyelitis risk factors differed between the tibia, femur, and upper extremity groups, sustaining an amputation, use of antibiotic beads, and being injured in the earlier years of the study (before significant practice pattern changes) were consistent predictors. Other risk factors included GA fracture severity ≥IIIb, blast injuries, foreign body at fracture site (with/without orthopedic implant), moderate/severe muscle damage and/or necrosis, and moderate/severe skin/soft-tissue damage. For upper extremity open fractures, initial stabilization following evacuation from the combat zone was associated with a reduced likelihood of osteomyelitis.
Conclusions: Forthcoming studies will examine the effectiveness of common antibiotic regimens for managing extremity deep soft-tissue infections to improve clinical outcomes of combat casualties and support development of clinical practice guidelines for CEWI treatment. The long-term impact of extremity trauma and resultant infections will be further investigated through both Department of Defense and Veterans Affairs follow-up, as well as examination of the impact on comorbidities and mental health/social factors.
Published by Oxford University Press on behalf of the Association of Military Surgeons of the United States 2022. This work is written by (a) US Government employee(s) and is in the public domain in the US.
Figures

References
-
- Belmont PJ Jr, Goodman GP, Zacchilli M, Posner M, Evans C, Owens BD: Incidence and epidemiology of combat injuries sustained during “the surge” portion of Operation Iraqi Freedom by a U.S. Army Brigade Combat Team. J Trauma 2010; 68(1): 204–10. - PubMed
-
- Belmont PJ, Owens BD, Schoenfeld AJ: Musculoskeletal injuries in Iraq and Afghanistan: epidemiology and outcomes following a decade of war. J Am Acad Orthop Surg 2016; 24(6): 341–8. - PubMed
-
- Owens BD, Kragh JF Jr, Macaitis J, Svoboda SJ, Wenke JC: Characterization of extremity wounds in Operation Iraqi Freedom and Operation Enduring Freedom. J Orthop Trauma 2007; 21(4): 254–7. - PubMed
-
- Schoenfeld AJ, Dunn JC, Bader JO, Belmont PJ Jr: The nature and extent of war injuries sustained by combat specialty personnel killed and wounded in Afghanistan and Iraq, 2003-2011. J Trauma Acute Care Surg 2013; 75(2): 287–91. - PubMed
-
- Krueger CA, Wenke JC, Ficke JR: Ten years at war: comprehensive analysis of amputation trends. J Trauma Acute Care Surg 2012; 73(6 Suppl 5): S438–44. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
