

DoD-VA Trauma Infection Research Collaboration
- PMID: 35512378
- PMCID: PMC9071422
- DOI: 10.1093/milmed/usab482
DoD-VA Trauma Infection Research Collaboration
Abstract
Background: In the aftermath of wars, there is a surge in the number of wounded service members who leave active duty and become eligible for healthcare through the Department of Veterans Affairs (VA). Collaborations between the Department of Defense (DoD) and VA are crucial to capture comprehensive data and further understand the long-term impact of battlefield trauma. We provide a summary of the development, methodology, and status of an effective collaboration between the Infectious Disease Clinical Research Program and the St. Louis VA Health Care System with the multicenter, observational Trauma Infectious Disease Outcomes Study (TIDOS), which examines the short- and long-term outcomes of deployment-related trauma.
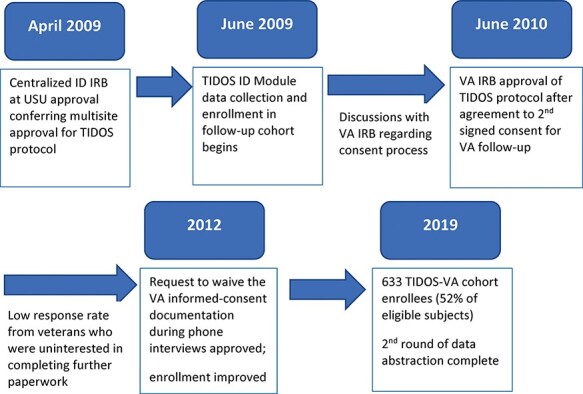
Methods: As part of TIDOS, wounded service members who transitioned to participating military hospitals in the United States (2009-2014) were given the opportunity to enroll in a prospective follow-up cohort study to continue to capture infection-related data after their hospital discharge. Enrollees in the TIDOS cohort who left military service and received health care through the VA also had the option of consenting to have relevant VA medical records abstracted and included with the study data. Infections considered to be complications resulting from the initial trauma were examined.
Results: Among 1,336 TIDOS enrollees, 1,221 (91%) registered and received health care through the VA with 633 (47%) consenting to follow-up using VA records and comprising the TIDOS-VA cohort. Of the first 337 TIDOS-VA cohort enrollees, 38% were diagnosed with a new trauma-related infection following hospital discharge (median: 88 days; interquartile range: 18-351 days). Approximately 71% of the infections were identified through DoD sources (medical records and follow-up) and 29% were identified through VA electronic medical records, demonstrating the utility of DoD-VA collaborations. The TIDOS DoD-VA collaboration has also been utilized to assess intermediate and long-term consequences of specific injury patterns. Among 89 TIDOS-VA cohort enrollees with genitourinary trauma, 36% reported sexual dysfunction, 21% developed at least one urinary tract infection, 14% had urinary retention/incontinence, and 8% had urethral stricture. The rate of urinary tract infections was 0.05/patient-year during DoD follow-up time and 0.07/patient-year during VA follow-up time.
Conclusions: Wider capture of infection-related outcome data through the DoD-VA collaboration provided a clearer picture of the long-term infection burden resulting from deployment-related trauma. Planned analyses include assessment of osteomyelitis among combat casualties with amputations and/or open fractures, evaluation of mental health and social factors related to injury patterns, and examination of health care utilization and cost in relation to infectious disease burdens.
Published by Oxford University Press on behalf of the Association of Military Surgeons of the United States 2022. This work is written by (a) US Government employee(s) and is in the public domain in the US.
Figures


References
-
- Congressional Research Service : U.S. periods of war and dates of recent conflicts. 2018. Available at https://fas.org/sgp/crs/natsec/RS21405.pdf; accessed July 6, 2021.
-
- Belmont PJ, Owens BD, Schoenfeld AJ: Musculoskeletal injuries in Iraq and Afghanistan: epidemiology and outcomes following a decade of war. J Am Acad Orthop Surg 2016; 24(6): 341–8. - PubMed
-
- Krueger CA, Wenke JC, Ficke JR: Ten years at war: comprehensive analysis of amputation trends. J Trauma Acute Care Surg 2012; 73(6 Suppl 5): S438–44. - PubMed
-
- Ficke JR, Eastridge BJ, Butler F, et al.: Dismounted complex blast injury report of the Army Dismounted Complex Blast Injury Task Force. J Trauma Acute Care Surg 2012; 73(6 Suppl 5): S520–34.
-
- Nessen SC, Gurney J, Rasmussen TE, et al.: Unrealized potential of the US Military battlefield trauma system: DOW rate is higher in Iraq and Afghanistan than in Vietnam, but CFR and KIA rate are lower. J Trauma Acute Care Surg 2018; 85(1S): S4–12. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
