

Effects of crystalloid and colloid priming strategies for cardiopulmonary bypass on colloid oncotic pressure and haemostasis: a meta-analysis
- PMID: 35512381
- PMCID: PMC9419694
- DOI: 10.1093/icvts/ivac127
Effects of crystalloid and colloid priming strategies for cardiopulmonary bypass on colloid oncotic pressure and haemostasis: a meta-analysis
Abstract
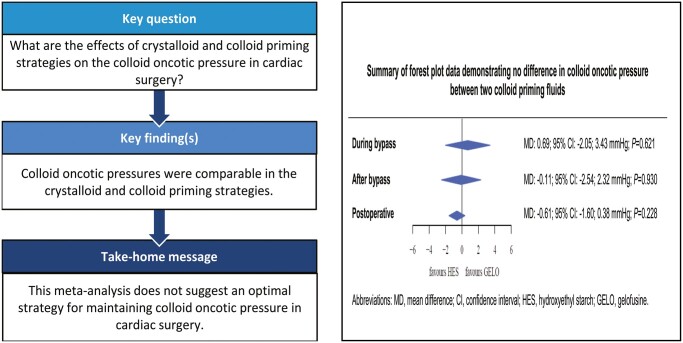
Objectives: Colloid oncotic pressure (COP) is an important factor in cardiac surgery, owing to its role in haemodilution. The effect of cardiopulmonary bypass prime fluids on the COP is unknown. In this study, the effect of crystalloid and colloid prime fluids, with or without retrograde autologous priming (RAP), on the COP during elective cardiac surgery was evaluated.
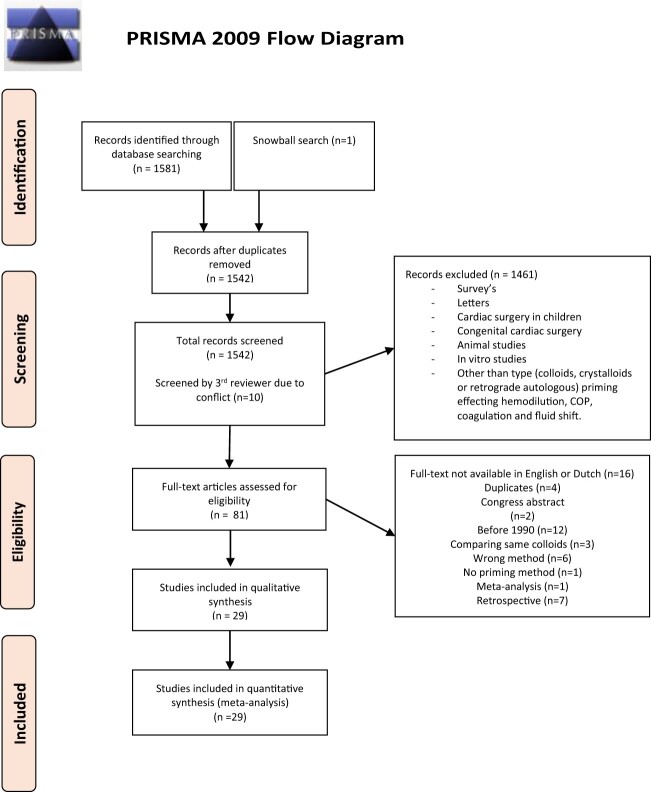
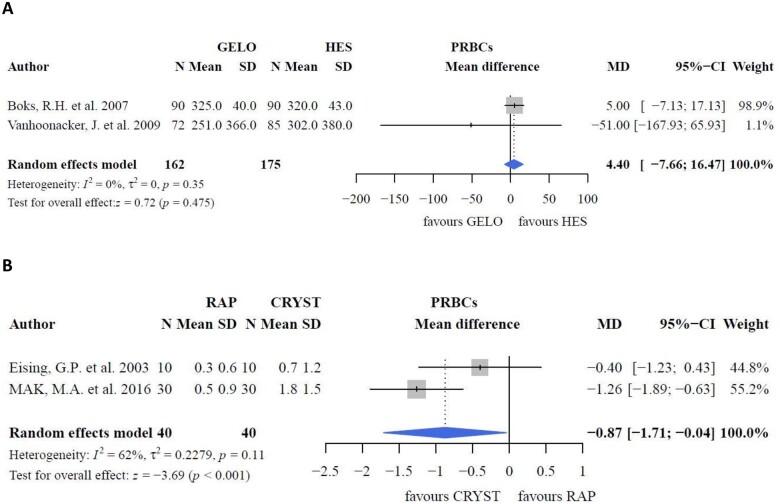
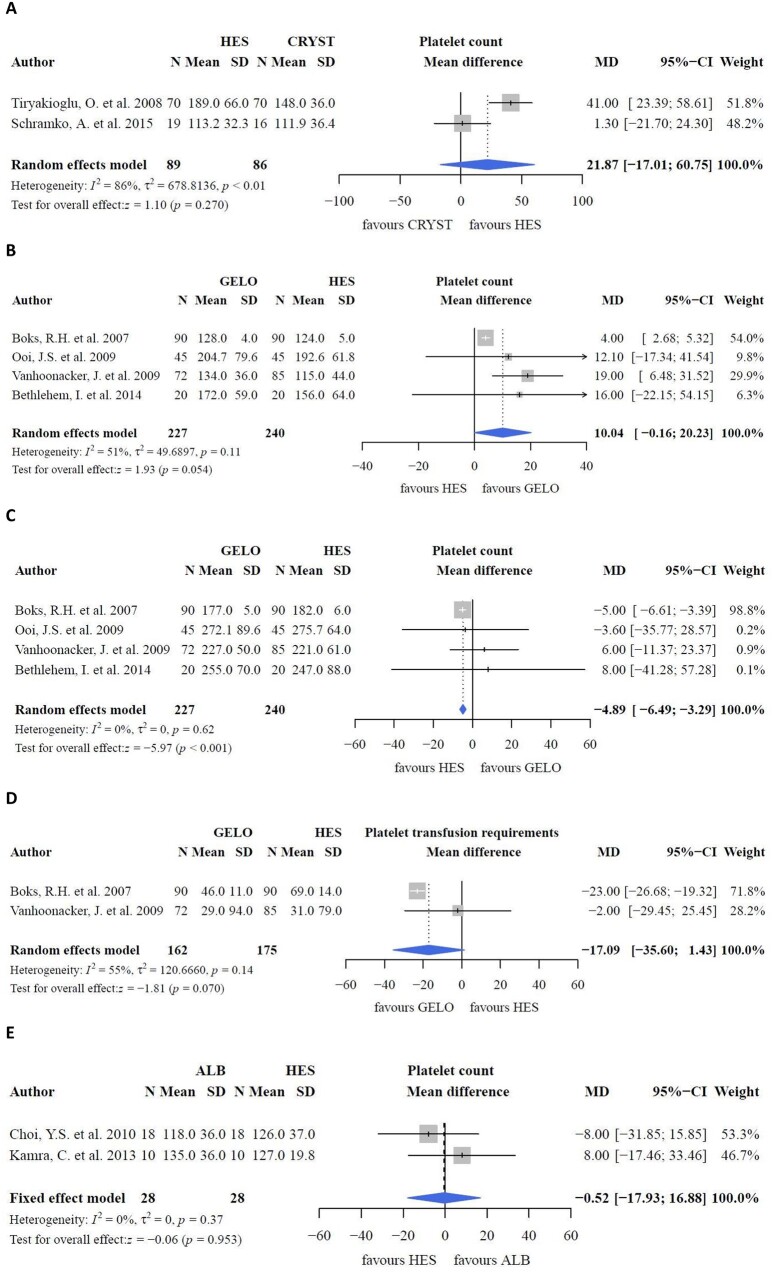
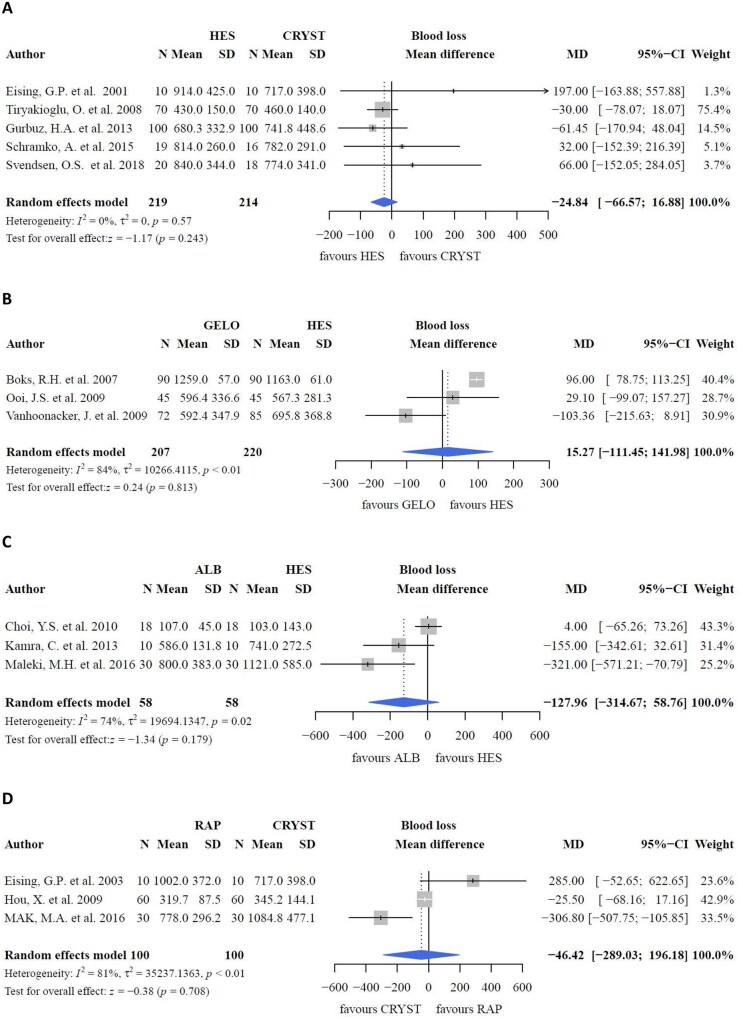
Methods: Randomized controlled trials and prospective clinical trials comparing crystalloid and colloid priming fluids or with RAP were selected. The primary outcome was the COP; secondary outcomes were fluid balance, fluid requirements, weight gain, blood loss, platelet count and transfusion requirements.
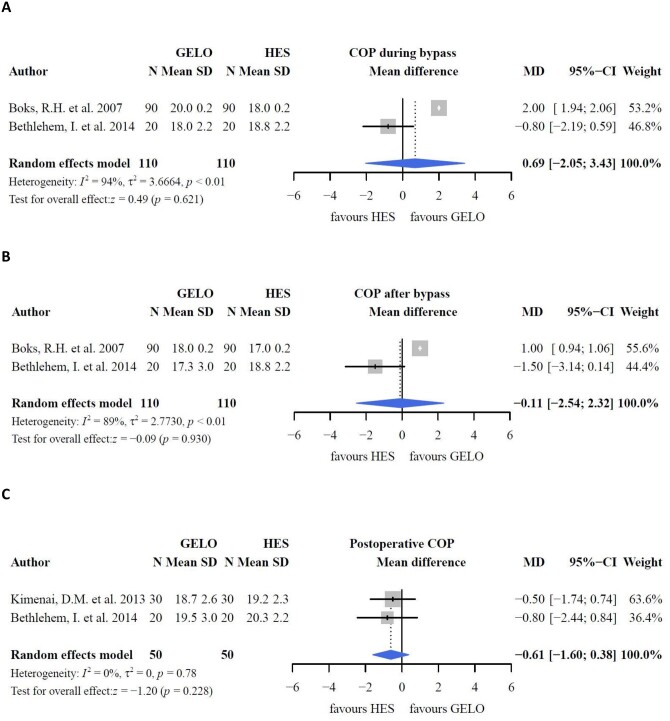
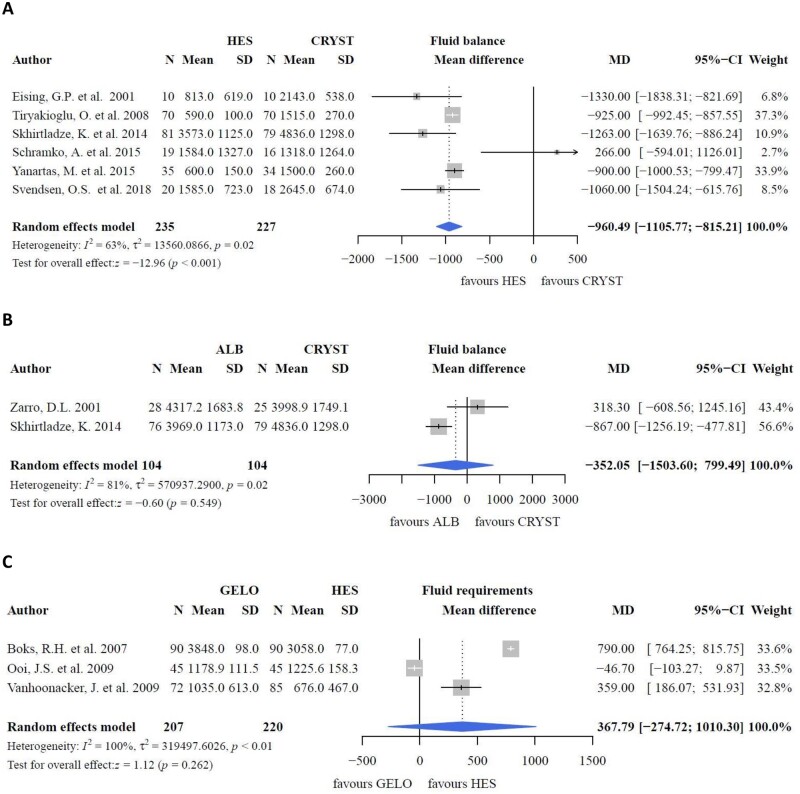
Results: From 1582 records, 29 eligible studies were identified. COPs were comparable between gelofusine and hydroxyethyl starch (HES) during bypass [mean difference (MD): 0.69; 95% confidence interval (CI): -2.05, 3.43; P = 0.621], after bypass (MD: -0.11; 95% CI: -2.54, 2.32; P = 0.930) and postoperative (MD: -0.61; 95% CI: -1.60, 0.38; P = 0.228). Fluid balance was lower with HES than with crystalloids. RAP reduced transfusion requirements compared with crystalloids. Blood loss was comparable between groups.
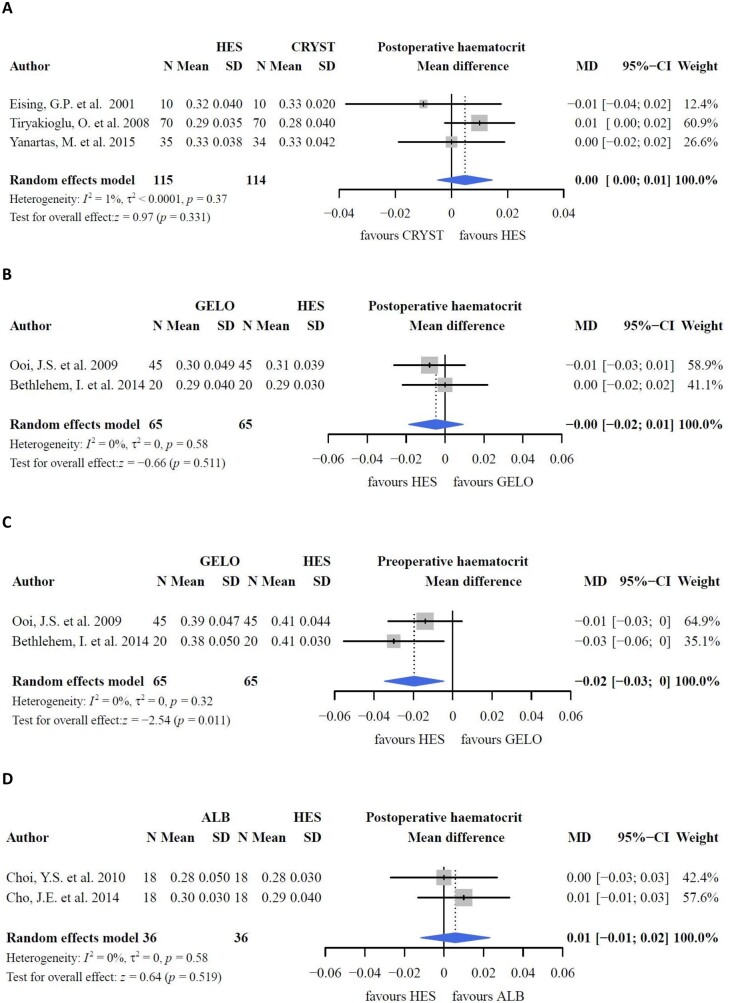
Conclusions: COPs did not differ between crystalloids and colloids. As a result of increased transcapillary fluid movement, fluid balance was lower with HES than with crystalloids. Haematocrit and transfusion requirements were comparable between groups. However, the latter was lower when RAP was applied to crystalloid priming compared with crystalloids alone. Finally, no differences in blood loss were observed between the groups.
Keywords: Cardiac surgery; Cardiopulmonary bypass; Colloid oncotic pressure; Prime fluid.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures
References
-
- Chappell D, Jacob M, Hofmann-Kiefer K, Conzen P, Rehm M.. A rational approach to perioperative fluid management. Anesthesiology 2008;109:723–40. - PubMed
-
- Scott DA, Hore PJ, Cannata J, Mason K, Treagus B, Mullaly J.. A comparison of albumin, polygeline and crystalloid priming solutions for cardiopulmonary bypass in patients having coronary artery bypass graft surgery. Perfusion 1995;10:415–24. - PubMed
-
- Alston RP, Theodosiou C, Sanger K.. Changing the priming solution from Ringer's to Hartmann's solution is associated with less metabolic acidosis during cardiopulmonary bypass. Perfusion 2007;22:385–9. - PubMed
-
- McIlroy DR, Kharasch ED.. Acute intravascular volume expansion with rapidly administered crystalloid or colloid in the setting of moderate hypovolemia. Anesth Analg 2003;96:1572–7. - PubMed
-
- Myers GJ, Legare JF, Sullivan JA, Leadon RB, Johnstone R, Swyer W. et al. Use of autologous blood as part of the perfusate for cardiopulmonary bypass: a priming technique. Perfusion 2002. 2002;17:211–6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
