

Axillary lymph node characteristics in breast cancer patients versus post-COVID-19 vaccination: Overview of current evidence per imaging modality
- PMID: 35512513
- PMCID: PMC9055782
- DOI: 10.1016/j.ejrad.2022.110334
Axillary lymph node characteristics in breast cancer patients versus post-COVID-19 vaccination: Overview of current evidence per imaging modality
Abstract
Background: Axillary lymph node characteristics on axillary ultrasound (US), breast MRI and 18F-FDG PET/CT are relevant at breast cancer diagnosis. Axillary lymphadenopathy after COVID-19 vaccination has been frequently reported. This may cause a diagnostic dilemma, particularly in the ipsilateral axilla in women who have a either a recent diagnosis of breast cancer or a history of breast cancer. This review provides an overview of the current evidence regarding axillary lymph node characteristics at breast cancer diagnosis versus "post-COVID-19 vaccination".
Methods: A non-systematic narrative review was performed. Studies describing axillary lymph node characteristics per imaging modality (axillary US, breast MRI and 18F-FDG PET/CT) in breast cancer patients versus post-COVID-19 vaccination were selected and used for the current study.
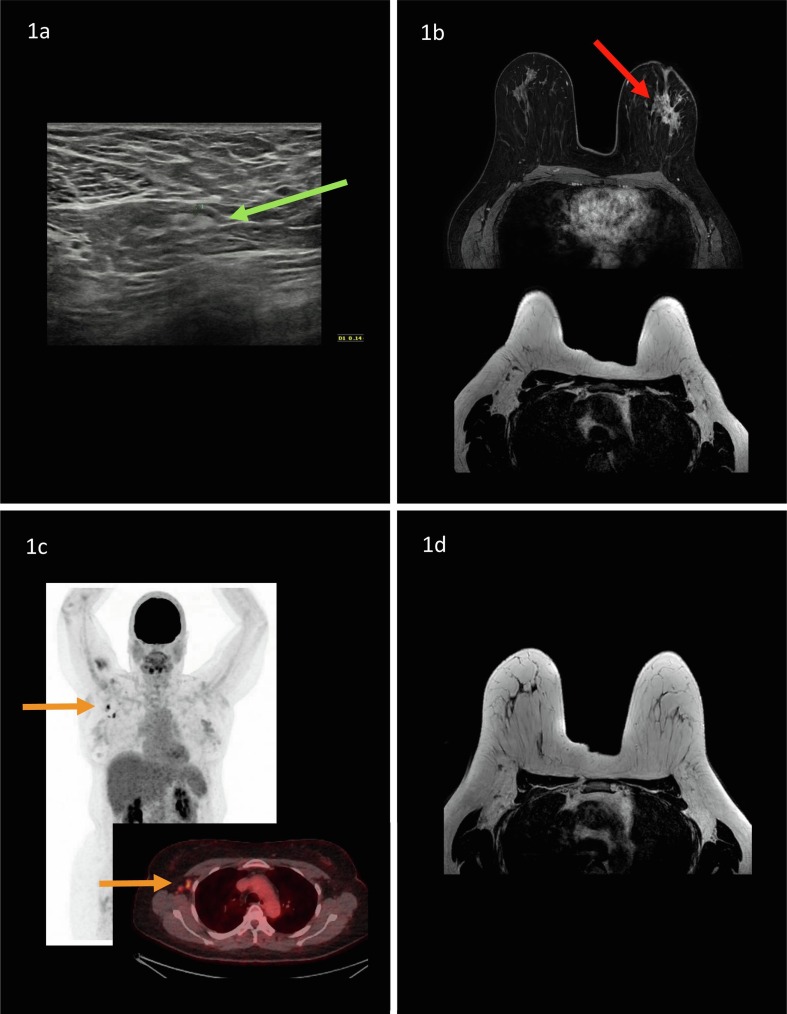
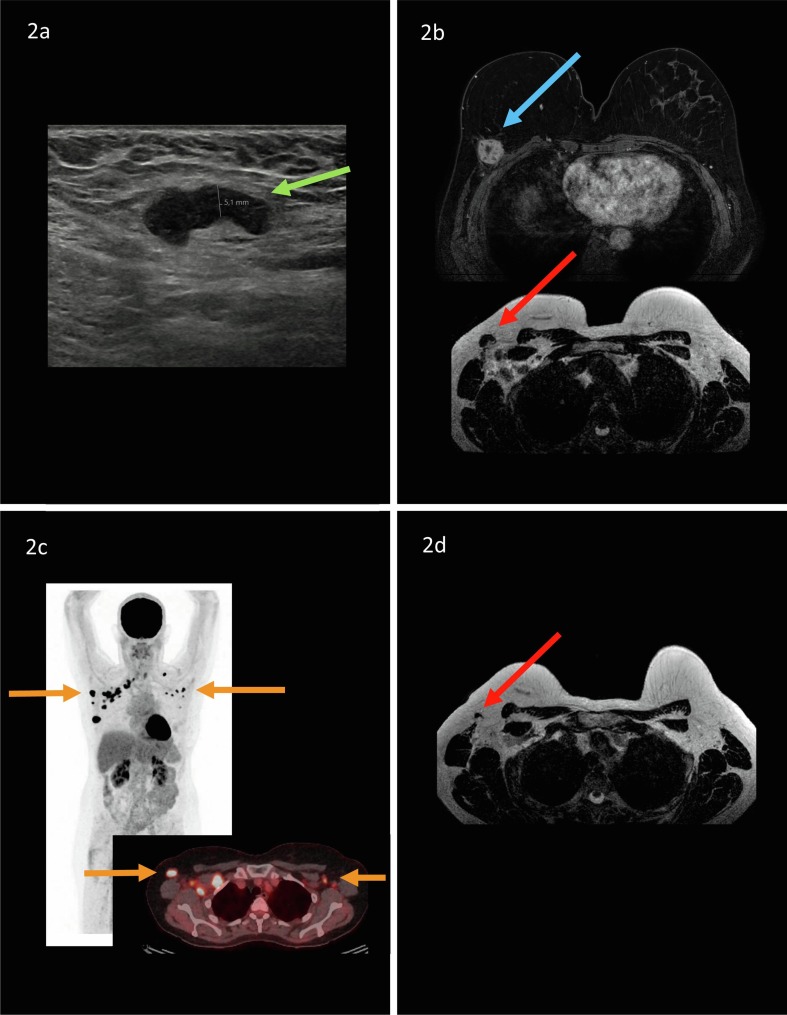
Results: The morphologic characteristics and distribution of abnormal nodes on US may differ from the appearance of metastatic adenopathy since diffuse cortical thickening of the lymph nodes is the most observed characteristic after vaccination, whereas metastases show as most suspicious characteristics focal cortical thickening and effacement of the fatty hilum. Current evidence on MRI and 18F-FDG on morphologic characteristics of axillary lymphadenopathy is missing, although it was suggested that vaccine related lymphadenopathy is more likely to be present in level 2 and 3 nodes than metastatic nodes. Reported frequencies of lymphadenopathy post-COVID-19 vaccination range from 49% to 85% (US), 29% (breast MRI) and 14.5% to 53.9% (18F-FDG PET/CT). Several factors may impact the presence or extent of lymphadenopathy post-COVID-19 vaccination: injection site, type of vaccine (i.e., mRNA versus vector), time interval (days) between vaccination and imaging, previous history of COVID-19 pneumonia, and first versus second vaccine dose.
Conclusion: Although lymph node characteristics differ at breast cancer diagnosis versus post-COVID-19 vaccination, clinical information regarding injection site, vaccine type and vaccination date needs to be documented to improve the interpretation and guide treatment towards the next steps of action.
Keywords: Axilla; Breast cancer; COVID-19 vaccination; Lymphadenopathy.
Copyright © 2022. Published by Elsevier B.V.
Figures
References
-
- Howlader N, Noone AM, Krapcho M, Garshell J, Neyman N, Altekruse SF, Kosary CL, Yu M, Ruhl J, Tatalovich Z, Cho H, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronins KA. SEER Cancer Statistics Review, 1975–2010, National Cancer Institue. Bethesda, MD, <https://seer.cancer.gov/archive/csr/1975_2010/>, based on November 2012 SEER data submission, posted to the SEER website, April 2013.
-
- Cardoso F., Kyriakides S., Ohno S., Penault-Llorca F., Poortmans P., Rubio I.T., Zackrisson S., Senkus E., Committee E.G. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019;30(10):1674. - PubMed
-
- A. Evans, R.M. Trimboli, A. Athanasiou, C. Balleyguier, P.A. Baltzer, U. Bick, J. Camps Herrero, P. Clauser, C. Colin, E. Cornford, E.M. Fallenberg, M.H. Fuchsjaeger, F.J. Gilbert, T.H. Helbich, K. Kinkel, S.H. Heywang-Kobrunner, C.K. Kuhl, R.M. Mann, L. Martincich, P. Panizza, F. Pediconi, R.M. Pijnappel, K. Pinker, S. Zackrisson, G. Forrai, F. Sardanelli, w.l.r.b.E.D.-T.E.B.C.C. European Society of Breast Imaging, Breast ultrasound: recommendations for information to women and referring physicians by the European Society of Breast Imaging, Insights Imag. 9(4) (2018) 449–461. - PMC - PubMed
-
- Chang J.M., Leung J.W.T., Moy L., Ha S.M., Moon W.K. Axillary nodal evaluation in breast cancer: state of the art. Radiology. 2020;295(3):500–515. - PubMed
-
- Bai H.X., Hsieh B., Xiong Z., Halsey K., Choi J.W., Tran T.M.L., Pan I., Shi L.B., Wang D.C., Mei J., Jiang X.L., Zeng Q.H., Egglin T.K., Hu P.F., Agarwal S., Xie F.F., Li S., Healey T., Atalay M.K., Liao W.H. Performance of radiologists in differentiating COVID-19 from non-COVID-19 viral pneumonia at chest CT. Radiology. 2020;296(2):E46–E54. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
