

Antithrombotic Therapy After Left Atrial Appendage Occlusion in Patients With Atrial Fibrillation
- PMID: 35512858
- PMCID: PMC9097170
- DOI: 10.1016/j.jacc.2022.02.047
Antithrombotic Therapy After Left Atrial Appendage Occlusion in Patients With Atrial Fibrillation
Abstract
Background: Pivotal trials of percutaneous left atrial appendage occlusion (LAAO) used specific postprocedure treatment protocols.
Objectives: This study sought to evaluate patterns of postprocedure care after LAAO with the Watchman device in clinical practice and compare the risk of adverse events for different discharge antithrombotic strategies.
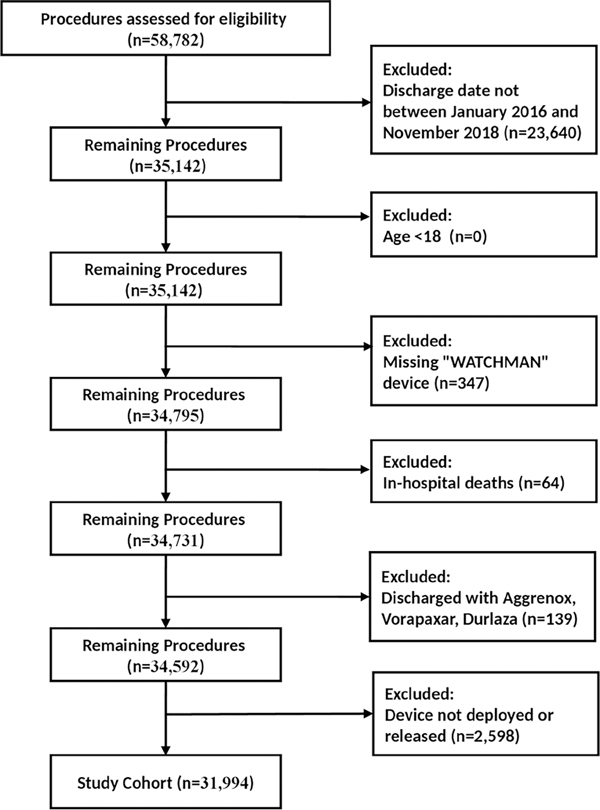
Methods: We evaluated patients in the LAAO Registry of the National Cardiovascular Data Registry who underwent LAAO with the Watchman device between 2016 and 2018. We assessed adherence to the full postprocedure trial protocol including standardized follow-up, imaging, and antithrombotic agents and then evaluated the most commonly used antithrombotic strategies and compared the rates and risk of adverse events at 45 days and 6 months by means of multivariable COX frailty regression.
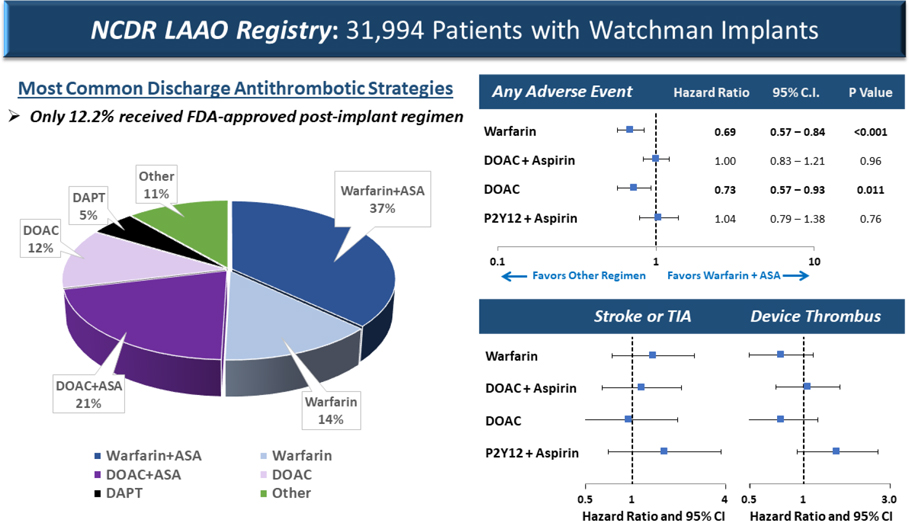
Results: Among 31,994 patients undergoing successful LAAO, only 12.2% received the full postprocedure treatment protocol studied in pivotal trials; the most common protocol deviations were with discharge antithrombotic medications. The most common discharge medication strategies were warfarin and aspirin (36.9%), direct oral anticoagulant (DOAC) and aspirin (20.8%), warfarin only (13.5%), DOAC only (12.3%), and dual antiplatelet therapy (5.0%). In multivariable Cox frailty regression, the adjusted risk of any adverse event through the 45-day follow-up visit were significantly lower for discharge on warfarin alone (HR: 0.692; 95% CI: 0.569-0.841) and DOAC alone (HR: 0.731; 95% CI: 0.574-0.930) compared with warfarin and aspirin. Warfarin alone retained lower risk at the 6-month follow-up.
Conclusions: In contemporary U.S. practice, practitioners rarely used the full U.S. Food and Drug Administration-approved postprocedure treatment protocols studied in pivotal trials of the Watchman device. Discharge after implantation on warfarin or DOAC without concomitant aspirin was associated with lower risk of adverse outcomes.
Keywords: anticoagulation; antiplatelet; bleeding; stroke.
Copyright © 2022 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This study was funded by the American College of Cardiology (ACC) National Cardiovascular Data Registry (NCDR) and the National Heart, Lung, and Blood Institute (NHLBI) grants R56HL142765 and R01HL142765. Dr Freeman has received salary support from the ACC NCDR and the NHLBI; and has received consulting/advisory board fees from Boston Scientific, Medtronic, Janssen Pharmaceuticals, and Biosense Webster. Dr Friedman has received educational grants from Boston Scientific, Medtronic, and Abbott; has received research grants from the NCDR, Boston Scientific, Abbott, Medtronic, and Biosense Webster; and has received consulting fees from Abbott and AtriCure. Dr Gibson has served as a consultant for Boston Scientific, Abbott, and Biosense Webster. Dr Goldsweig has received grant support from the National Institute of General Medical Sciences (1U54GM115458) and the Center for Heart and Vascular Research, University of Nebraska Medical Center. Dr Price has received consulting/advisory board fees from Boston Scientific, Medtronic, Abbott Vascular, W.L. Gore Medical, and Conformal Medical; has received speaker’s fees from Chiesi USA; and has received research grants (to institution) from Daiichi-Sankyo. Dr Reddy is an unpaid consultant to and has received grant support from Boston Scientific; has served as a consultant for Abbott, Ablacon, Acutus Medical, Affera, Apama Medical, Aquaheart, Atacor, Autonomix, Axon Therapeutics, Backbeat, BioSig, Biosense-Webster, Biotronik, Cardiac Implants, CardiaCare, Cardiofocus, Cardionomic, CardioNXT/AFTx, Circa Scientific, Corvia Medical, Dinova-Hangzhou Nuomao Medtech Co, Ltd, East End Medical, EBR, EPD, Epix Therapeutics, EpiEP, Eximo, Farapulse, Fire1, Impulse Dynamics, HRT, Intershunt, Javelin, Kardium, Keystone Heart, LuxMed, Medlumics, Medtronic, Middlepeak, Nuvera, Philips, Pulse Biosciences, Sirona Medical, Thermedical, and Valcare; and has equity in Ablacon, Acutus Medical, Affera, Apama Medical, Aquaheart, Atacor, Autonomix, Axon Therapeutics, Backbeat, BioSig, Cardiac Implants, CardiaCare, Circa Scientific, Corvia Medical, Dinova-Hangzhou Nuomao Medtech Co, Ltd, East End Medical, EPD, Epix Therapeutics, EpiEP, Eximo, Farapulse, HRT, Intershunt, Javelin, Kardium, Keystone Heart, LuxMed, Manual Surgical Sciences, Middlepeak, Newpace, Nuvera, Sirona Medical, Surecor, Valcare, and Vizaramed. Dr Masoudi has received an institutional contract with the ACC for his role as Chief Scientific Advisor of the NCDR. Dr Curtis has received an institutional contract with the ACC for his role as Senior Scientific Advisor of the NCDR. Dr Doshi has received research grants (to institution) and consulting/advisory board fees from Boston Scientific, Biosense Webster, Conformal Medical, Terumo, and Abbott Vascular. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Antithrombotic Therapy After Left Atrial Appendage Occlusion: Cornucopia and Gertrude Stein.J Am Coll Cardiol. 2022 May 10;79(18):1799-1801. doi: 10.1016/j.jacc.2022.03.328. J Am Coll Cardiol. 2022. PMID: 35512859 No abstract available.
References
-
- Blackshear JL, Odell JA. Appendage obliteration to reduce stroke in cardiac surgical patients with atrial fibrillation. Ann Thorac Surg 1996;61:755–759. - PubMed
-
- Stoddard MF, Dawkins PR, Prince CR, Ammash NM. Left atrial appendage thrombus is not uncommon in patients with acute atrial fibrillation and a recent embolic event: a transesophageal echocardiographic study. J Am Coll Cardiol 1995;25:452–9. - PubMed
-
- Jain AK, Gallagher S. Percutaneous occlusion of the left atrial appendage in non-valvular atrial fibrillation for the prevention of thromboembolism: NICE guidance. Heart 2011;97:762–765. - PubMed
-
- Bartus K, Bednarek J, Myc J, et al. Feasibility of closed-chest ligation of the left atrial appendage in humans. Heart Rhythm 2011;8:188–193. - PubMed
-
- Fountain R, Holmes DR Jr, Hodgson PK, Chandrasekaran K, Van Tassel R, Sick P. Potential applicability and utilization of left atrial appendage occlusion devices in patients with atrial fibrillation. Am Heart J 2006;152:720–723. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
