

High-Intensity Statin Use Among Patients With Atherosclerosis in the U.S
- PMID: 35512860
- PMCID: PMC9344279
- DOI: 10.1016/j.jacc.2022.02.048
High-Intensity Statin Use Among Patients With Atherosclerosis in the U.S
Abstract
Background: Preventive therapy among patients with established atherosclerotic cardiovascular disease (ASCVD) is generally underused. Whether new guideline recommendations and a focus on implementation have improved the use of high-intensity statins is unknown.
Objectives: This study sought to evaluate the patterns and predictors of statin use among patients with ASCVD.
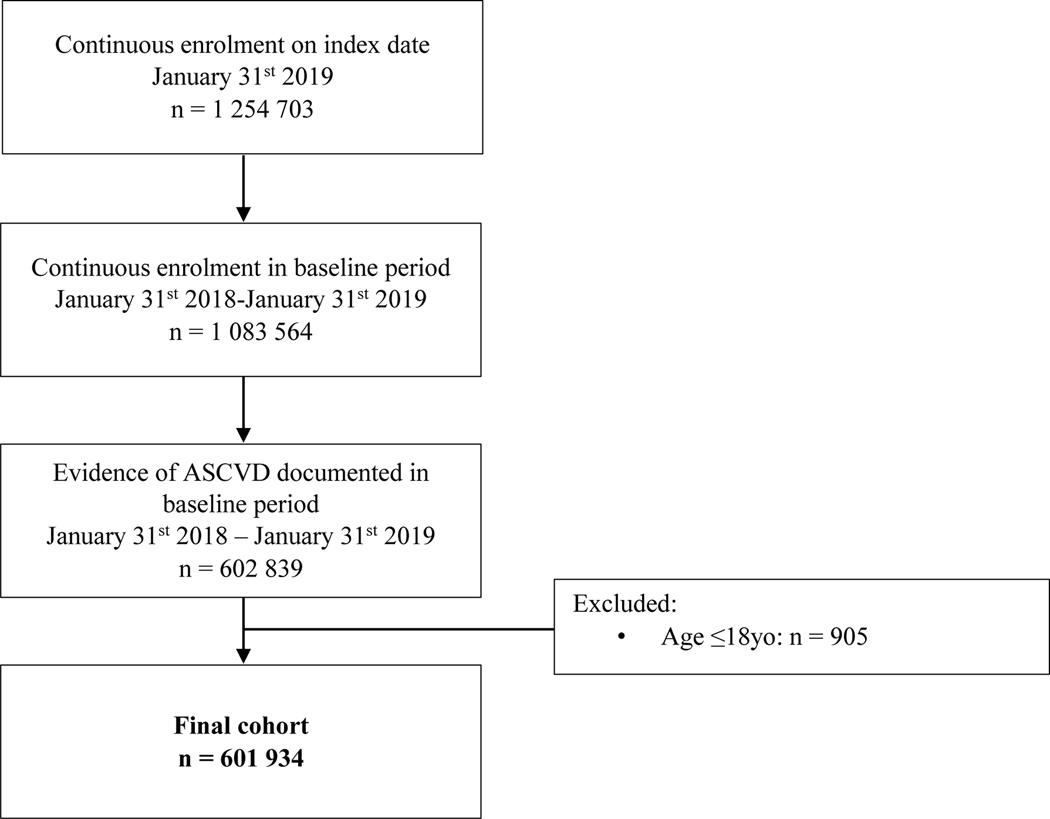
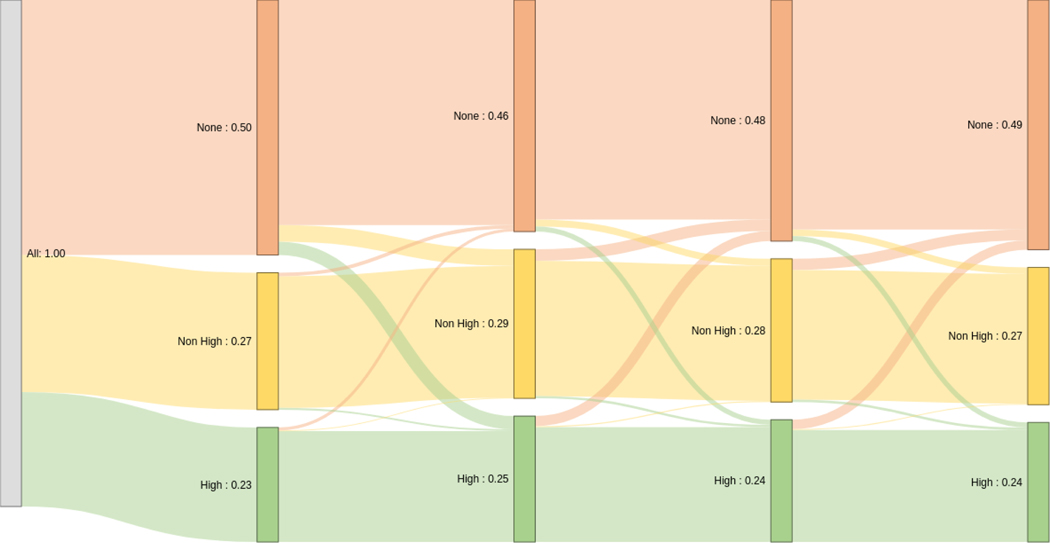
Methods: In this retrospective cohort study, pharmacy and medical claims data from a commercial health plan were queried for patients with established ASCVD between January 31, 2018, and January 31, 2019. Statin use on an index date of January 31, 2019, was evaluated, as was 12-month adherence and discontinuation. Multivariable logistic regression was used to determine independent associations with statin use of varying intensities.
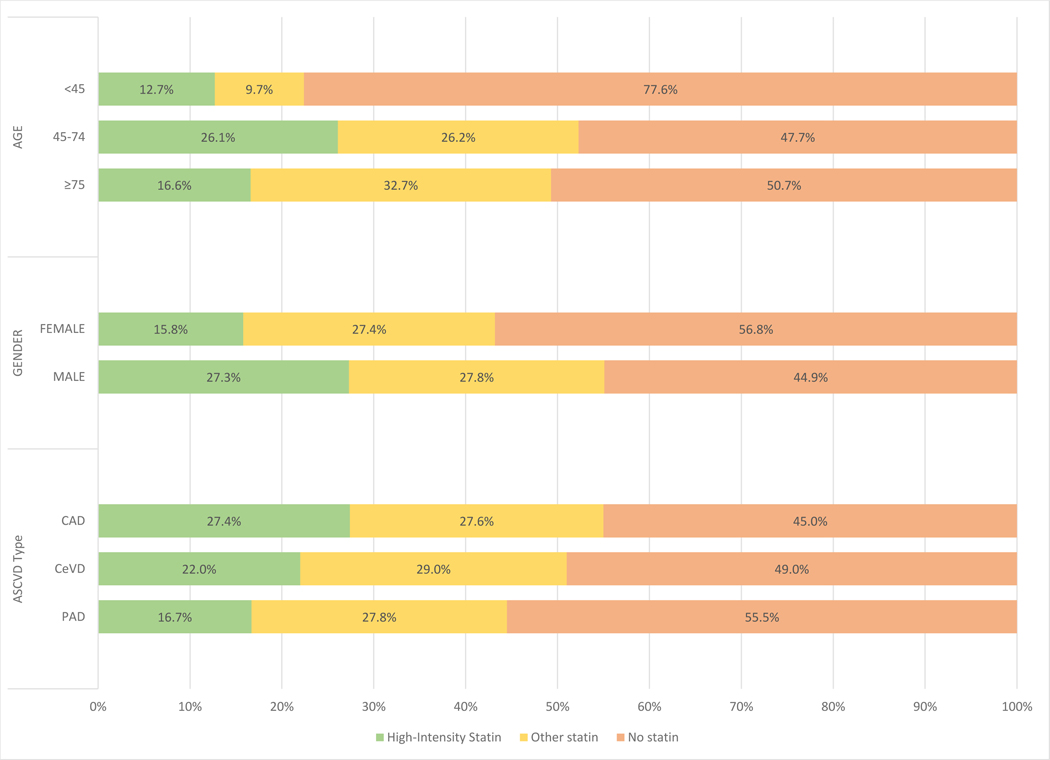
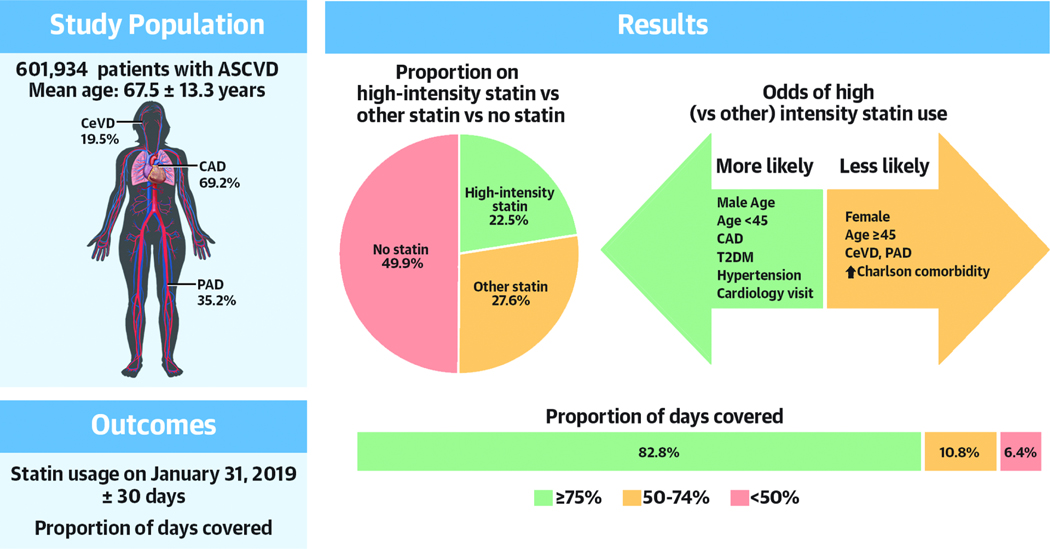
Results: Of the 601,934 patients with established ASCVD, 41.7% were female, and the mean age was 67.5 ± 13.3 years. Overall, 22.5% of the cohort were on a high-intensity statin, 27.6% were on a low- or moderate-intensity statin, and 49.9% were not on any statin. In multivariable analysis, younger patients, female patients, and those with higher Charlson comorbidity score were less likely to be prescribed any statin. Among statin users, female patients, older patients, and those with peripheral artery disease were less likely to be on a high-intensity formulation, whereas a cardiology encounter in the prior year increased the odds. The majority of high-intensity stain users achieved high levels of adherence.
Conclusions: Substantial underuse of statins persists in a large, insured, and contemporary cohort of patients with ASCVD from the United States. In particular, concerning gaps in appropriate statin use remain among younger patients, women, and those with noncoronary ASCVD.
Keywords: atherosclerosis; predictors; prevention; secondary prevention; statins.
Copyright © 2022 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Dr Nelson has received grants from Diabetes Australia and the Royal Australasian College of Physicians. Dr Haynes is an employee of HealthCore, a subsidiary of Anthem. Dr Shambhu is an employee of HealthCore, a subsidiary of Anthem. Dr Eapen is a previous employee of HealthCore. Dr Cziraky is an employee of HealthCore, a subsidiary of Anthem. Dr Nanna has received funding from the American College of Cardiology Foundation supported by the George F. and Ann Harris Bellows Foundation, and from the National Institute on Aging/National Institutes of Health from R03AG074067 (GEMSSTAR award). Dr Calvert is supported by U.S. Food and Drug Administration grant U18FD005292 and Clinical Trials Transformation Initiative membership fees. Dr Gallagher is an employee of HealthCore. Dr Pagidipati has received grants from Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Novartis, Novo Nordisk, Regeneron, Sanofi, Verily Life Sciences; and has received consulting fees from Boehringer Ingelheim, Eli Lilly, AstraZeneca, and Novo Nordisk. Dr Granger has received research grants and consulting/speaker fees from Boehringer Ingelheim, Bristol Myers Squibb, Janssen Pharmaceutica Products, LP, and Pfizer; has received research grants from AKROS, Apple, AstraZeneca, Daichii-Sankyo, U.S. Food and Drug Administration, GlaxoSmithKline, Medtronic Foundation, and Novartis Pharmaceutical Company; and has received consulting/speaker fees from AbbVie, Bayer Corp US, Boston Scientific Corp, CeleCor Therapeutics, Correvio, Espero BioPharma, Medscape, Medtronic Inc, Merck, National Institutes of Health, Novo Nordisk, Rhoshan Pharmaceuticals, and Roche Diagnostics.
Figures
Comment in
-
Guideline-Concordant Statin Therapy Use in Secondary Prevention: Should the Medical Community Wait for Divine Intervention?J Am Coll Cardiol. 2022 May 10;79(18):1814-1817. doi: 10.1016/j.jacc.2022.02.042. J Am Coll Cardiol. 2022. PMID: 35512861 No abstract available.
-
High-Dose Statins Increase Adverse Events and Do Not Improve Survival.J Am Coll Cardiol. 2022 Oct 18;80(16):e125. doi: 10.1016/j.jacc.2022.06.045. J Am Coll Cardiol. 2022. PMID: 36229095 No abstract available.
-
Reply: High-Dose Statins Increase Adverse Events and Do Not Improve Survival.J Am Coll Cardiol. 2022 Oct 18;80(16):e127. doi: 10.1016/j.jacc.2022.08.741. J Am Coll Cardiol. 2022. PMID: 36229096 No abstract available.
References
-
- Lloyd-Jones DM, Leip EP, Larson MG et al. Prediction of lifetime risk for cardiovascular disease by risk factor burden at 50 years of age. Circulation 2006;113:791–8. - PubMed
-
- Collins R, Reith C, Emberson J et al. Interpretanttion of the evidence for the efficacy and safety of statin therapy. Lancet 2016;388:2532–2561. - PubMed
-
- Cannon CP, Braunwald E, McCabe CH et al. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med 2004;350:1495–504. - PubMed
-
- LaRosa JC, Grundy SM, Waters DD et al. Intensive lipid lowering with atorvastatin in patients with stable coronary disease. N Engl J Med 2005;352:1425–35. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
