

Mortality Outcomes by Fibrosis Stage in Nonalcoholic Fatty Liver Disease: A Systematic Review and Meta-analysis
- PMID: 35513235
- PMCID: PMC10792524
- DOI: 10.1016/j.cgh.2022.04.014
Mortality Outcomes by Fibrosis Stage in Nonalcoholic Fatty Liver Disease: A Systematic Review and Meta-analysis
Abstract
Background & aims: Fibrosis is a key determinant of clinical outcomes in nonalcoholic fatty liver disease (NAFLD), but time-dependent risk of mortality has not been reported in previous meta-analyses. We performed an updated time-to-event meta-analysis to provide robust estimates for all-cause and liver-related mortality in biopsy-confirmed NAFLD with comparisons between fibrosis stages.
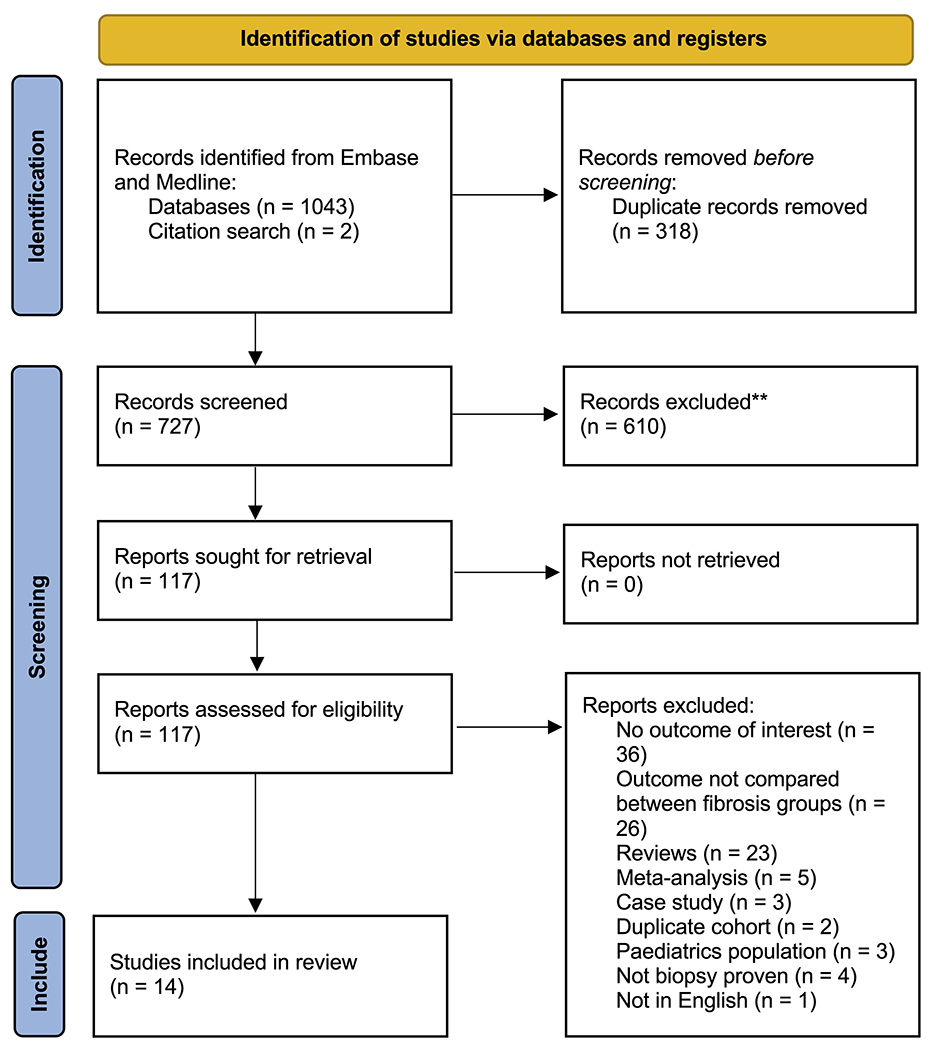
Methods: Medline and Embase databases were searched to include cohort studies reporting survival outcomes by fibrosis stage in biopsy-proven NAFLD. Survival estimates were pooled using reconstructed individual participant data. Conventional meta-analysis was conducted to pool adjusted hazard ratios (HRs) using DerSimonian and Laird random effects model.
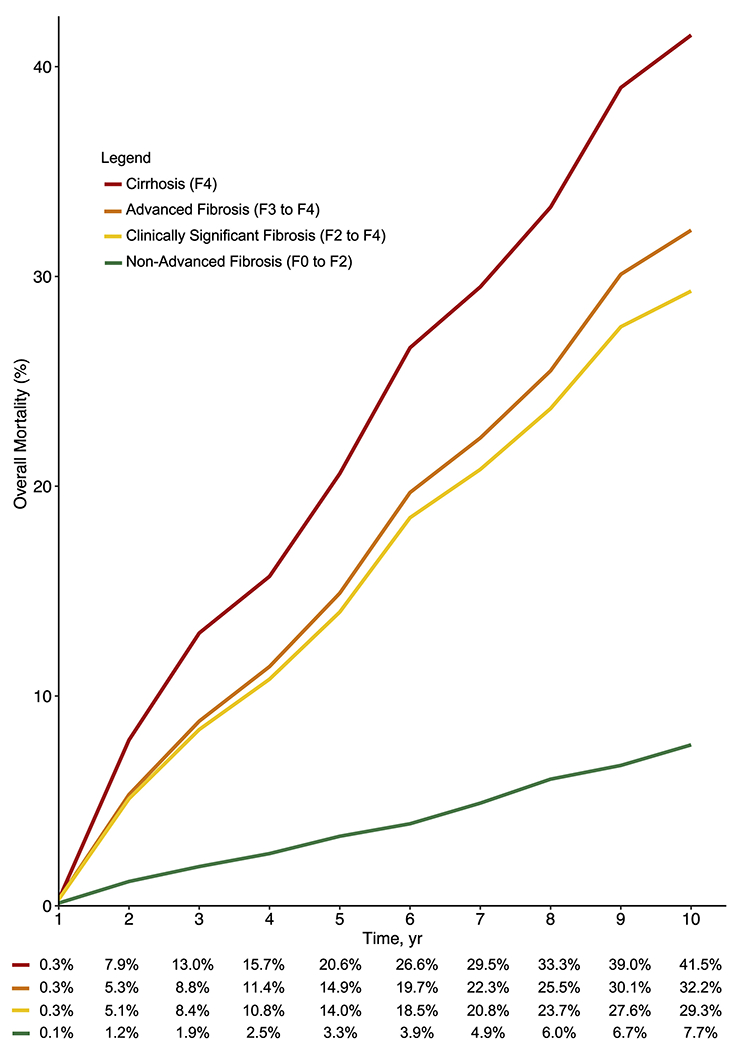
Results: A total of 14 articles involving 17,301 patients with NAFLD were included. All-cause mortality at 1, 5, and 10 years for stage 0 to 2 fibrosis was 0.1%, 3.3%, and 7.7% vs 0.3%, 20.6%, and 41.5% for stage 4 fibrosis. Compared with stage 0 fibrosis, all-cause mortality increased with fibrosis stage: stage 2; HR, 1.46 (95% confidence interval [CI], 1.08-1.98), stage 3; HR, 1.96 (95% CI, 1.41-2.72), and stage 4; HR, 3.66 (95% CI, 2.65-5.05). Risk for liver-related mortality increased exponentially as fibrosis stage increased: stage 2; HR, 4.07 (95% CI, 1.44-11.5), stage 3; HR, 7.59 (95% CI, 2.80-20.5), and stage 4; HR, 15.1 (95% CI, 5.27-43.4). Stage 3 to 4 fibrosis had a higher all-cause (HR, 3.32) and liver-related mortality (HR, 10.40) compared with stage 0 to 2 fibrosis, whereas stage 4 fibrosis had higher all-cause (HR, 2.67; 95% CI, 1.47-4.83) and liver-related mortality (HR, 2.57; 95% CI, 1.22-5.42) vs stage 3 fibrosis.
Conclusions: Risk of all-cause and liver-related mortality increases substantially with fibrosis stage. These data have important implications for prognostication and trial design.
Keywords: Disease Progression; Fibrosis; Liver Disease; Mortality.
Copyright © 2023 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
These authors disclose the following: Rohit Loomba serves as a consultant or advisory board member for Anylam/Regeneron, Arrowhead Pharmaceuticals, AstraZeneca, Bristol-Myer Squibb, CohBar, Eli Lilly, Galmed, Gilead, Glympse Bio, Inipharm, Intercept, Ionis, Janssen Inc, Merck, Metacrine Inc, NGM Biopharmaceuticals, Novartis, Novo Nordisk, Pfizer, Promethera, Sagimet, 89 Bio, and Viking Therapeutics. In addition, his institution has received grant support from Allergan, Boehringer-Ingelheim, Bristol-Myers Squibb, Cirius, Eli Lilly and Company, Galectin Therapeutics, Galmed Pharmaceuticals, GE, Genfit, Gilead, Intercept, Inventiva, Janssen, Madrigal Pharmaceuticals, Merck, NGM Biopharmaceuticals, Pfizer, pH Pharma, and Siemens. He is also co-founder of Liponexus, Inc. Daniel Q. Huang serves as an advisory board member for Eisai. The remaining authors disclose no conflicts.
Figures
References
-
- Younossi ZM, Koenig AB, Abdelatif D, et al. Global epidemiology of nonalcoholic fatty liver disease: meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016;64:73–84. - PubMed
-
- Lim GEH, Tang A, Ng CH, et al. An observational data meta-analysis on the differences in prevalence and risk factors between MAFLD vs NAFLD. Clin Gastroenterol Hepatol 2021:Online ahead of print. - PubMed
-
- Muthiah MD, Cheng Han N, Sanyal AJ. A clinical overview of non-alcoholic fatty liver disease: a guide to diagnosis, the clinical features, and complications– what the non-specialist needs to know. Diabetes Obes Metab 2022;24(Suppl 2):3–14. - PubMed
-
- Muthiah MD, Sanyal AJ. Burden of disease due to nonalcoholic fatty liver disease. Gastroenterol Clin North Am 2020;49:1–23. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
