

Therapeutic and tectonic keratoplasty with simple cryopreserved remnants of donor corneas: an 11 year retrospective case series
- PMID: 35513446
- PMCID: PMC9069216
- DOI: 10.1038/s41598-022-10994-3
Therapeutic and tectonic keratoplasty with simple cryopreserved remnants of donor corneas: an 11 year retrospective case series
Abstract
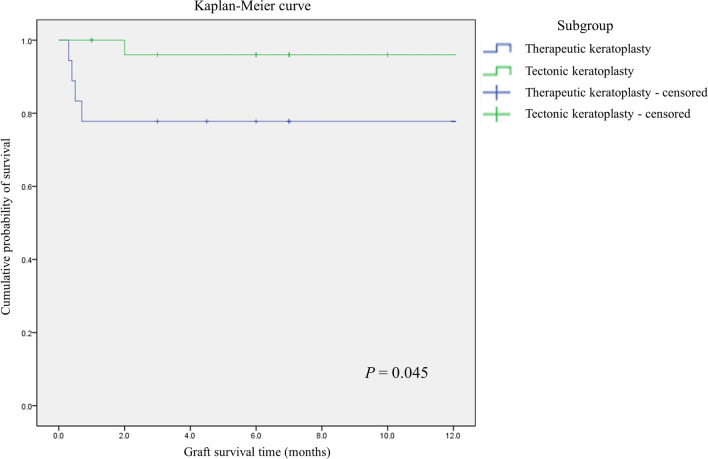
This study sought to describe the use of deep-frozen donor corneal remnants preserved after keratoplasty procedures for therapeutic or tectonic keratoplasty without subsequent optical keratoplasty. This single-center retrospective consecutive case series analyzed the electronic medical records of patients who had undergone therapeutic or tectonic keratoplasty using deep-frozen donor remains preserved in Optisol-GS, for the past 11 years at Keimyung University Dongsan Medical Center. Fifty-five surgical cases in 46 patients were included. Twenty-three surgical cases in 18 patients underwent therapeutic keratoplasty for refractory infectious corneal ulcer. Complete eradication of primary infection was achieved in 14 patients (77.8%). Tectonic keratoplasty were performed 32 cases in 28 patients. Twenty-seven of 28 patients were ultimately able to maintain anatomical integrity (96.4%). Mean uncorrected visual acuity improved from 1.77 ± 0.94 preoperatively to 1.31 ± 0.95 at the last follow-up postoperatively in the tectonic graft group by logarithm of the minimal angle of resolution (P = 0.002). There were no cases of graft rejection. Keratoplasty using cryopreserved donor tissue is a suitable surgical alternative for infectious or non-infectious corneal ulcers in elderly patients or patients with poor general condition. It could be a viable alternative to overcome the shortage of corneal donors.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Small, overlapping tectonic keratoplasty involving graft-host junction of penetrating keratoplasty.Am J Ophthalmol. 2000 Apr;129(4):465-7. doi: 10.1016/s0002-9394(99)00413-4. Am J Ophthalmol. 2000. PMID: 10764854
-
Tectonic deep anterior lamellar keratoplasty in impending corneal perforation using cryopreserved cornea.Korean J Ophthalmol. 2011 Apr;25(2):132-5. doi: 10.3341/kjo.2011.25.2.132. Epub 2011 Mar 11. Korean J Ophthalmol. 2011. PMID: 21461227 Free PMC article.
-
Tectonic Lamellar Keratoplasty Using Cryopreserved Cornea in a Large Descemetocele.Yonsei Med J. 2016 Jan;57(1):269-71. doi: 10.3349/ymj.2016.57.1.269. Yonsei Med J. 2016. PMID: 26632412 Free PMC article.
-
Cornea donors who have had prior refractive surgery: data from the Eye Bank Association of America.Curr Opin Ophthalmol. 2016 Jul;27(4):323-6. doi: 10.1097/ICU.0000000000000278. Curr Opin Ophthalmol. 2016. PMID: 27138639 Review.
-
Surgical alternatives to keratoplasty in microbial keratitis.Surv Ophthalmol. 2021 Mar-Apr;66(2):290-307. doi: 10.1016/j.survophthal.2020.08.004. Epub 2020 Aug 29. Surv Ophthalmol. 2021. PMID: 32866469 Review.
Cited by
-
Five years of emergency keratoplasty at a tertiary eye hospital.Int Ophthalmol. 2024 Nov 11;44(1):426. doi: 10.1007/s10792-024-03333-0. Int Ophthalmol. 2024. PMID: 39527140
-
Efficacy of Emergency Penetrating Keratoplasty with Cryopreserved Human Donor Corneas.Ophthalmol Ther. 2024 Apr;13(4):979-994. doi: 10.1007/s40123-024-00889-z. Epub 2024 Feb 12. Ophthalmol Ther. 2024. PMID: 38345711 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
