

A retrospective observational study of osteoporosis management after a fragility fracture in primary care
- PMID: 35513573
- PMCID: PMC9072526
- DOI: 10.1007/s11657-022-01110-z
A retrospective observational study of osteoporosis management after a fragility fracture in primary care
Abstract
In many countries, osteoporosis is predominantly managed by primary care physicians; however, management after a fragility fracture has not been widely investigated. We describe osteoporosis care gaps in a real-world patient cohort. Our findings help inform initiatives to identify and overcome obstacles to effective management of patients after fragility fracture.
Purpose: A fragility fracture is a major risk factor for subsequent fracture in adults aged ≥ 50 years. This retrospective observational study aimed to characterize post-fracture management in Canadian primary care.
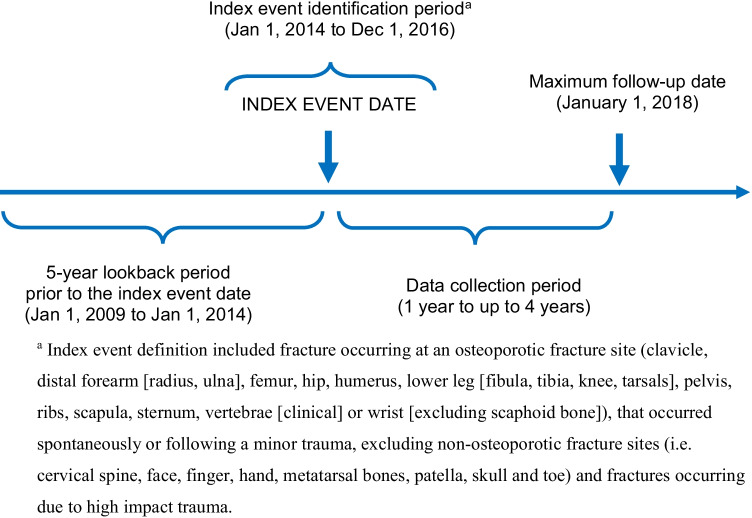
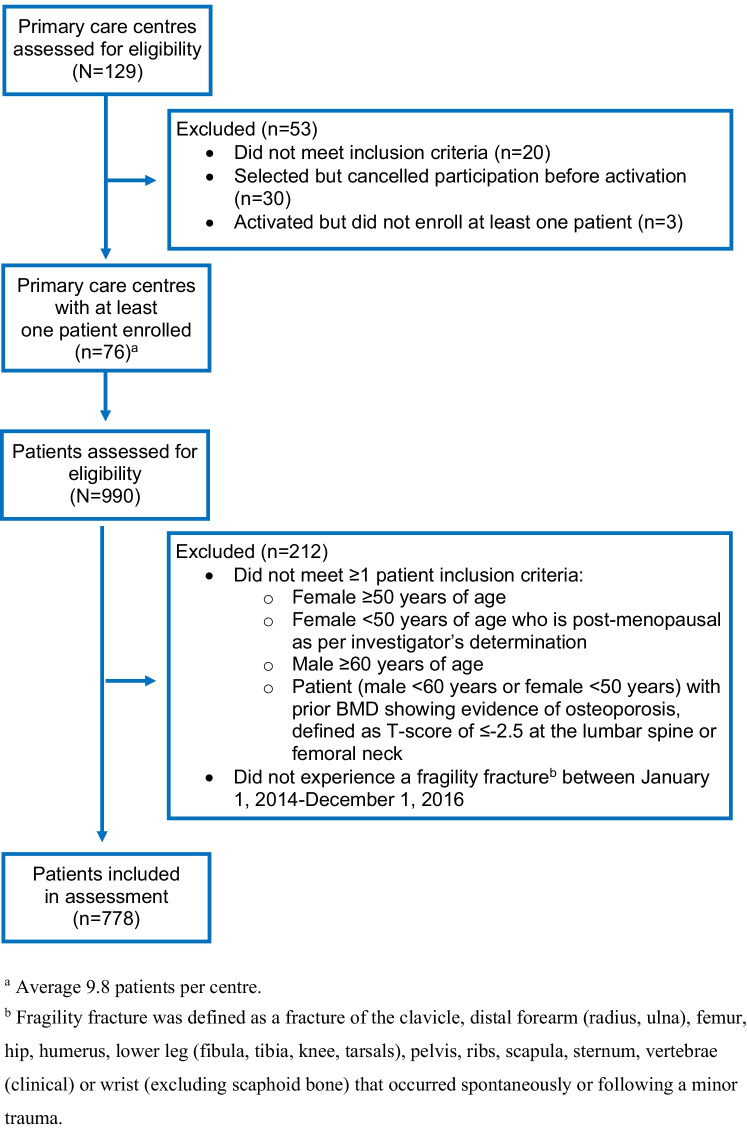
Methods: A total of 778 patients with an index fragility fracture (low-trauma, excluding small bones) occurring between 2014 and 2016 were identified from medical records at 76 primary care centers in Canada, with follow-up until January 2018.
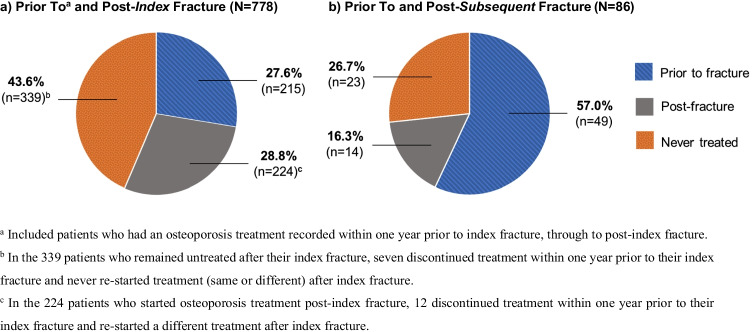
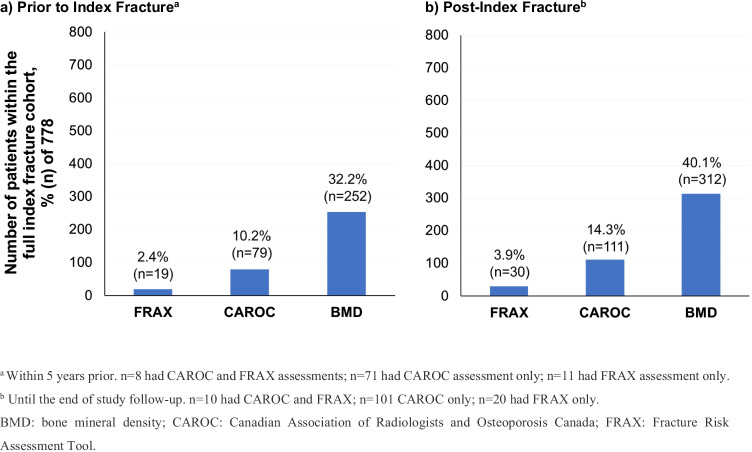
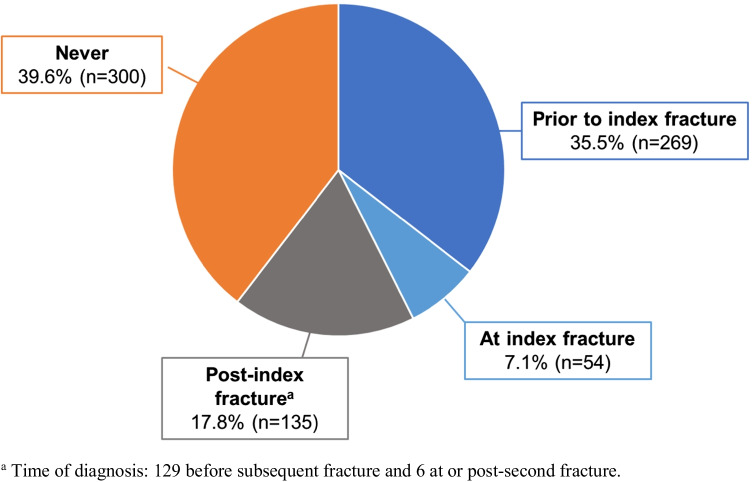
Results: Of 778 patients (80.5% female, median age [IQR] 73 [64-80]), 215 were on osteoporosis treatment and 269 had osteoporosis diagnosis recorded prior to their index fracture. The median follow-up was 363 (IQR 91-808) days. Of patients not on osteoporosis treatment at their index fracture, 60.2% (n = 339/563) remained untreated after their index fracture and 62.2% (n = 23/37) continued untreated after their subsequent fracture. After their index fracture, fracture risk assessment (FRAX or CAROC) was not performed in 83.2% (n = 647/778) of patients, and 59.9% (n = 466/778) of patients did not receive bone mineral density testing. Of patients without osteoporosis diagnosis recorded prior to their index date, 61.3% (n = 300/489) remained undiagnosed after their index fracture. At least one subsequent fracture occurred in 11.5% (n = 86/778) of patients.
Conclusion: In the primary care setting, fragility fracture infrequently resulted in osteoporosis treatment or fracture risk assessment, even after multiple fragility fractures. These results suggest a fragility fracture is not recognized as a major risk factor for subsequent fracture and its occurrence does not prompt primary care physicians to intervene. These data urge initiatives to identify and overcome obstacles to primary care physicians' effective management of patients after fragility fractures.
Keywords: Fracture; Osteoporosis; Primary care; Real-world data; Secondary prevention.
© 2022. The Author(s).
Conflict of interest statement
AB has received research grants, speaker honoraria, and/or consultancies from Amgen, AstraZeneca, Bausch Health, Bayer, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, HLS Therapeutics, Janssen, Novartis, Pfizer, Sanofi, and Spectrum Therapeutics. DLK has received research grants, speaker honoraria, and/or consultancies from Alexion, Amgen, BioSyent, and Radius Health. AAK has received research grants from Alexion, Amgen, Ascendis, Chugai, Radius Health, Takeda, and Ultragenyx. MS has received research grants, speaker honoraria, and/or consultancies from Amgen, Aspen, Astellas, Bayer, BioSyent, Duchesnay, GlaxoSmithKline, Merck, Mithra, Pfizer, Searchlight, Sprout, Sunovion, and Therapeutics MD. AM has received speaker honoraria and/or consultancies from Amgen, Eli Lilly, and Sanofi. MR, SMC, LS, and MP are/were employees at the time of study completion and own stock in Amgen. JPL declares no conflict of interest.
Figures
References
-
- Camacho PM, Petak SM, Binkley N, Diab DL, Eldeiry LS, Farooki A et al (2020) American Association of Clinical Endocrinologists/American College of Endocrinology clinical practice guidelines for the diagnosis and treatment of postmenopausal osteoporosis: 2020 update. Endocr Pract 26(1 Suppl):1–46. 10.4158/gl-2020-0524suppl - PubMed
-
- Khan AA, Choudur HN, Lentle B (2020) Diagnosis of osteoporosis: clinical and densitometric analysis. Can Assoc Radiol J 72(2):326. 10.1177/0846537120944385 - PubMed
-
- International Osteoporosis Foundation. About osteoporosis. Available from: https://www.osteoporosis.foundation/health-professionals/about-osteoporosis. Accessed 2 Feb 2021
-
- Giangregorio L, Papaioannou A, Cranney A, Zytaruk N, Adachi JD (2006) Fragility fractures and the osteoporosis care gap: an international phenomenon. Semin Arthritis Rheum 35(5):293-305. 10.1016/j.semarthrit.2005.11.001 - PubMed
-
- Public Health Agency of Canada. Osteoporosis and related fractures in Canada: report from the Canadian Chronic Disease Surveillance System, 2020. https://www.canada.ca/en/public-health/services/publications/diseases-co.... Accessed 15 Jan 2021
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
