

Biomechanical properties of a suture anchor system from human allogenic mineralized cortical bone matrix for rotator cuff repair
- PMID: 35513813
- PMCID: PMC9069722
- DOI: 10.1186/s12891-022-05371-0
Biomechanical properties of a suture anchor system from human allogenic mineralized cortical bone matrix for rotator cuff repair
Abstract
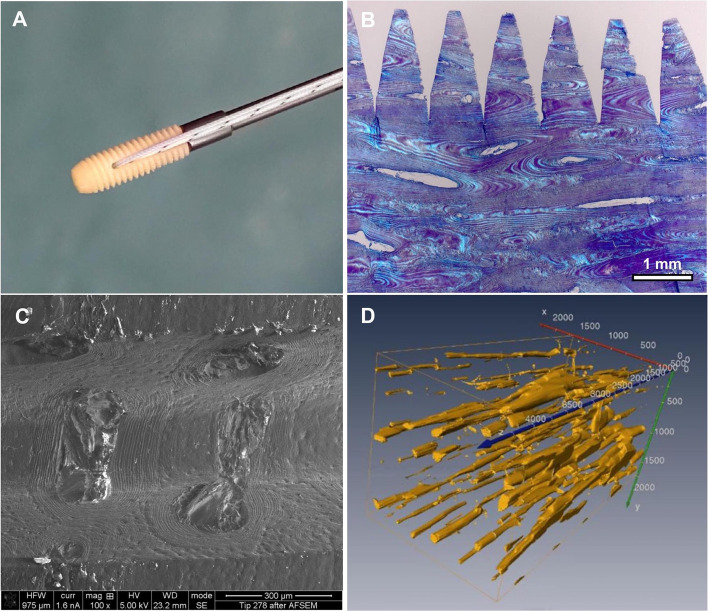
Background: Suture anchors (SAs) made of human allogenic mineralized cortical bone matrix are among the newest developments in orthopaedic and trauma surgery. Biomechanical properties of an allogenic mineralized suture anchor (AMSA) are not investigated until now. The primary objective was the biomechanical investigation of AMSA and comparing it to a metallic suture anchor (MSA) and a bioabsorbable suture anchor (BSA) placed at the greater tuberosity of the humeral head of cadaver humeri. Additionally, we assessed the biomechanical properties of the SAs with bone microarchitecture parameters.
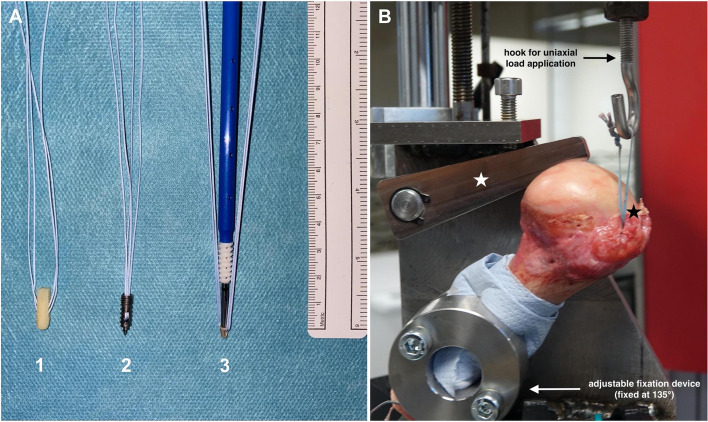
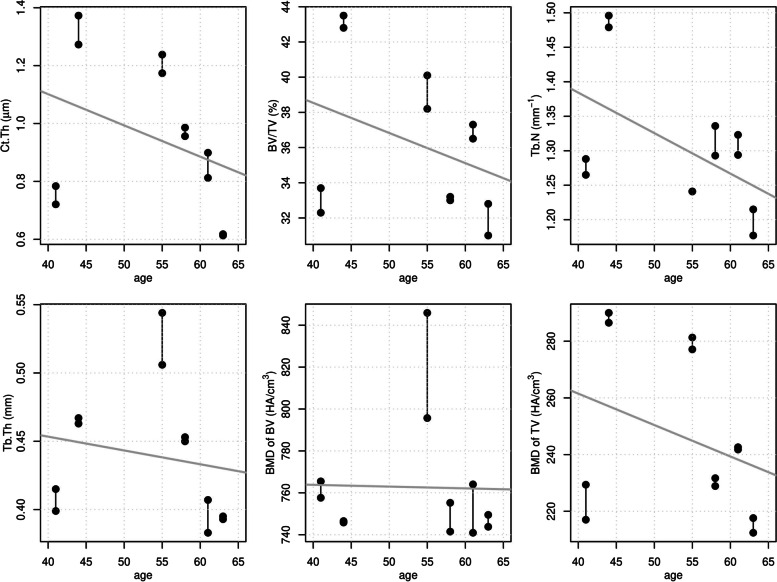
Methods: First, bone microarchitecture of 12 fresh frozen human cadaver humeri from six donors was analyzed by high-resolution peripheral quantitative computed tomography. In total, 18 AMSAs, 9 MSAs, and 9 BSAs were implanted at a 60° angle. All three SA systems were systematically implanted alternating in three positions within the greater tuberosity (position 1: anterior, position 2: central, position 3: posterior) with a distance of 15 mm to each other. Biomechanical load to failure was measured in a uniaxial direction at 135°.
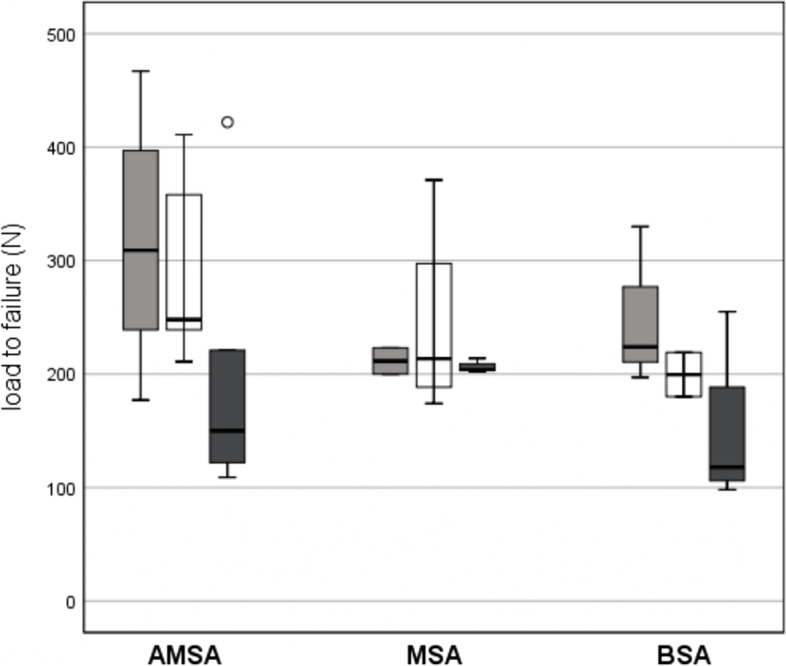
Results: Mean age of all specimens was 53.6 ± 9.1 years. For all bone microarchitecture measurements, linear regression slope estimates were negative which implies decreasing values with increasing age of specimens. Positioning of all three SA systems at the greater tuberosity was equally distributed (p = 0.827). Mean load to failure rates were higher for AMSA compared to MSA and BSA without reaching statistical significance between the groups (p = 0.427). Anchor displacement was comparable for all three SA systems, while there were significant differences regarding failure mode between all three SA systems (p < 0.001). Maximum load to failure was reached in all cases for AMSA, in 44.4% for MSA, and in 55.6% for BSA. Suture tear was observed in 55.6% for MSA and in 22.2% for BSA. Anchor breakage was solely seen for BSA (22.2%). No correlations were observed between bone microarchitecture parameters and load to failure rates of all three suture anchor systems.
Conclusions: The AMSA showed promising biomechanical properties for initial fixation strength for RCR. Since reduced BMD is an important issue for patients with chronic rotator cuff lesions, the AMSA is an interesting alternative to MSA and BSA. Also, the AMSA could improve healing of the enthesis.
Keywords: Allogenic mineralized suture anchor; Biomechanical analysis; High-resolution peripheral quantitative computed tomography; Rotator cuff reconstruction; Shoulder; Shoulder surgery; Suture anchor.
© 2022. The Author(s).
Conflict of interest statement
KP is Chief Executive Officer and Medical Director of surgebright. EP is Vice Medical Director of surgebright. JES, BOP, GS, PRH, BL, CM, CF, RM, JG, IF certify that he or she have no commercial associations (e.g., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
Figures
Similar articles
-
A novel suture anchor constructed of cortical bone for rotator cuff repair: a biomechanical study on sheep humerus specimens.Int Orthop. 2016 Sep;40(9):1913-8. doi: 10.1007/s00264-016-3185-4. Epub 2016 Apr 8. Int Orthop. 2016. PMID: 27055449
-
Pullout strength of standard vs. cement-augmented rotator cuff repair anchors in cadaveric bone.Clin Biomech (Bristol). 2018 May;54:132-136. doi: 10.1016/j.clinbiomech.2018.03.016. Epub 2018 Mar 20. Clin Biomech (Bristol). 2018. PMID: 29587146
-
Biomechanical Analysis of Medial-Row All-Suture Suture Anchor Fixation for Rotator Cuff Repair in a Pair-Matched Cadaveric Model.Arthroscopy. 2019 May;35(5):1370-1376. doi: 10.1016/j.arthro.2019.01.023. Epub 2019 Apr 15. Arthroscopy. 2019. PMID: 31000387
-
Biomechanical Strength of Rotator Cuff Repairs: A Systematic Review and Meta-regression Analysis of Cadaveric Studies.Am J Sports Med. 2019 Jul;47(8):1984-1993. doi: 10.1177/0363546518780928. Epub 2018 Jul 5. Am J Sports Med. 2019. PMID: 29975549
-
Biochemical and biomechanical influence on peri anchor cyst formation in rotator cuff repair.Acta Orthop Belg. 2022 Dec;88(4):713-718. doi: 10.52628/88.4.10793. Acta Orthop Belg. 2022. PMID: 36800654 Review.
Cited by
-
Attaching artificial Achilles and tibialis cranialis tendons to bone using suture anchors in a rabbit model: assessment of outcomes.PeerJ. 2025 Jan 21;13:e18756. doi: 10.7717/peerj.18756. eCollection 2025. PeerJ. 2025. PMID: 39866575 Free PMC article.
-
Advanced strategies for constructing interfacial tissues of bone and tendon/ligament.J Tissue Eng. 2022 Dec 23;13:20417314221144714. doi: 10.1177/20417314221144714. eCollection 2022 Jan-Dec. J Tissue Eng. 2022. PMID: 36582940 Free PMC article. Review.
References
-
- Teunis T, Lubberts B, Reilly BT, Ring D. A systematic review and pooled analysis of the prevalence of rotator cuff disease with increasing age. J Shoulder Elb Surg. 2014;23:1913–1921. - PubMed
-
- Moosmayer S, Lund G, Seljom US, Haldorsen B, Svege IC, Hennig T, et al. At a 10-year follow-up, tendon repair is superior to physiotherapy in the treatment of small and medium-sized rotator cuff tears. J Bone Joint Surg Am. 2019;101-A:1050–1060. - PubMed
-
- Collin P, Colmar M, Thomazeau H, Mansat P, Boileau P, Valenti P, et al. Clinical and MRI outcomes 10 years after repair of massive Posterosuperior rotator cuff tears. J Bone Joint Surg Am. 2018;100-A:1854–1863. - PubMed
-
- Heuberer PR, Smolen D, Pauzenberger L, Plachel F, Salem S, Laky B, et al. Longitudinal long-term magnetic resonance imaging and clinical follow-up after single-row arthroscopic rotator cuff repair clinical superiority of structural tendon integrity. Am J Sports Med. 2017;45:1283–1288. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
