

Timing of invasive strategy in non-ST-elevation acute coronary syndrome: a meta-analysis of randomized controlled trials
- PMID: 35514079
- PMCID: PMC9433309
- DOI: 10.1093/eurheartj/ehac213
Timing of invasive strategy in non-ST-elevation acute coronary syndrome: a meta-analysis of randomized controlled trials
Abstract
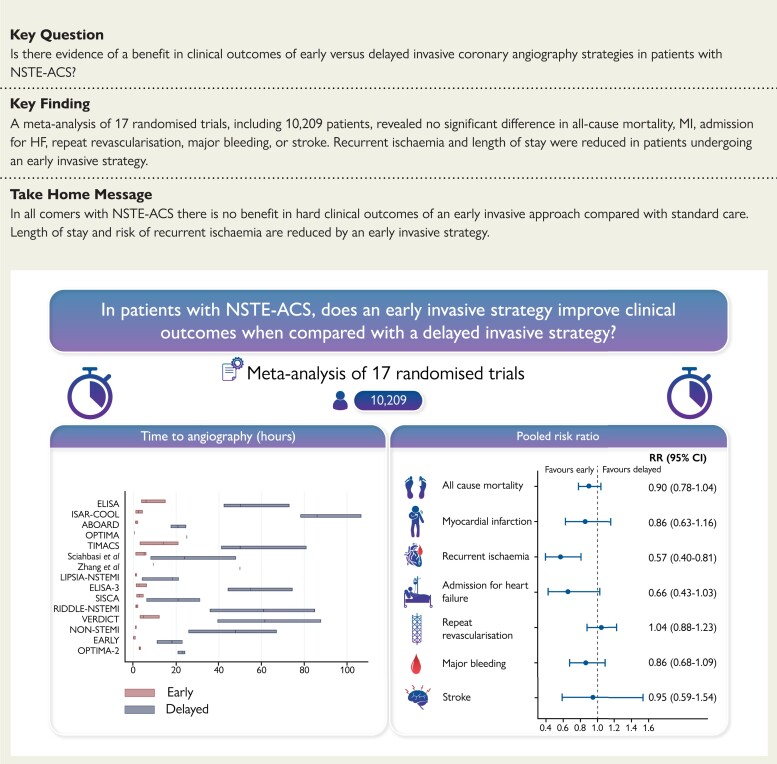
Aims: The optimal timing of an invasive strategy (IS) in non-ST-elevation acute coronary syndrome (NSTE-ACS) is controversial. Recent randomized controlled trials (RCTs) and long-term follow-up data have yet to be included in a contemporary meta-analysis.
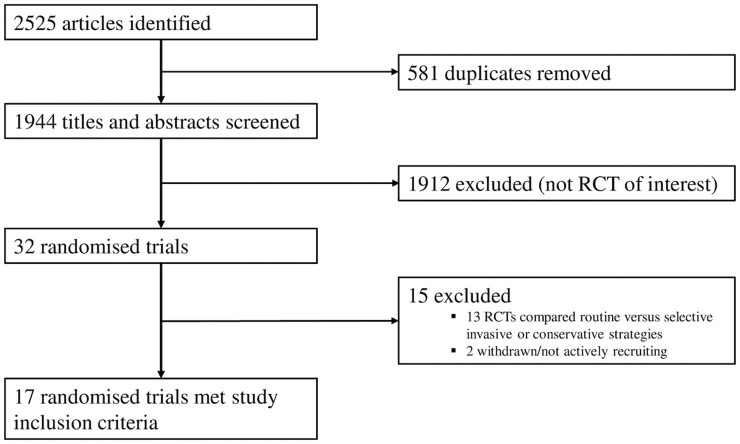
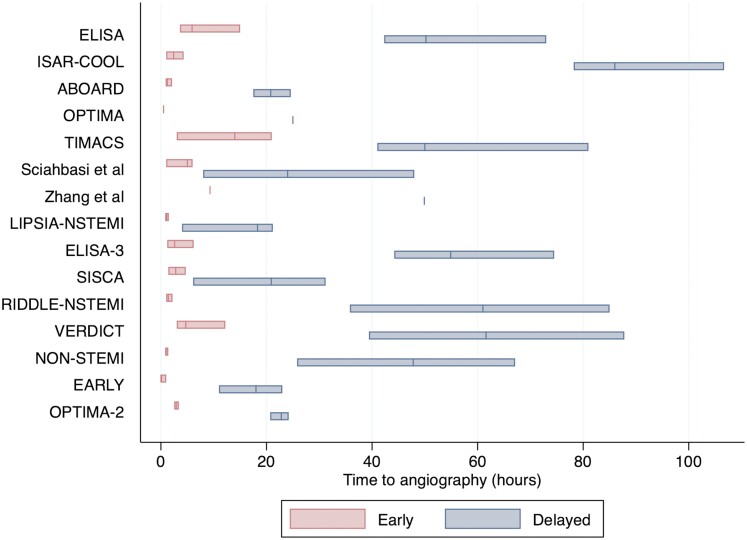
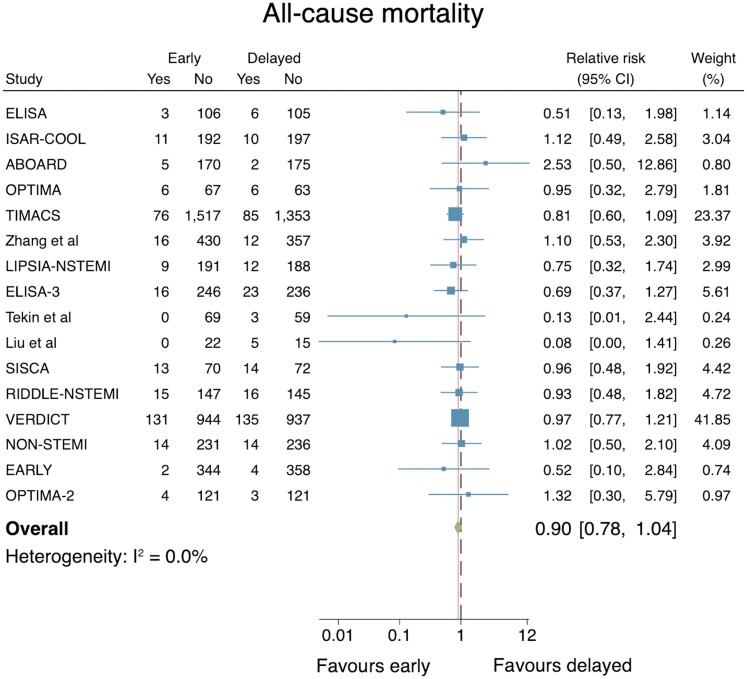
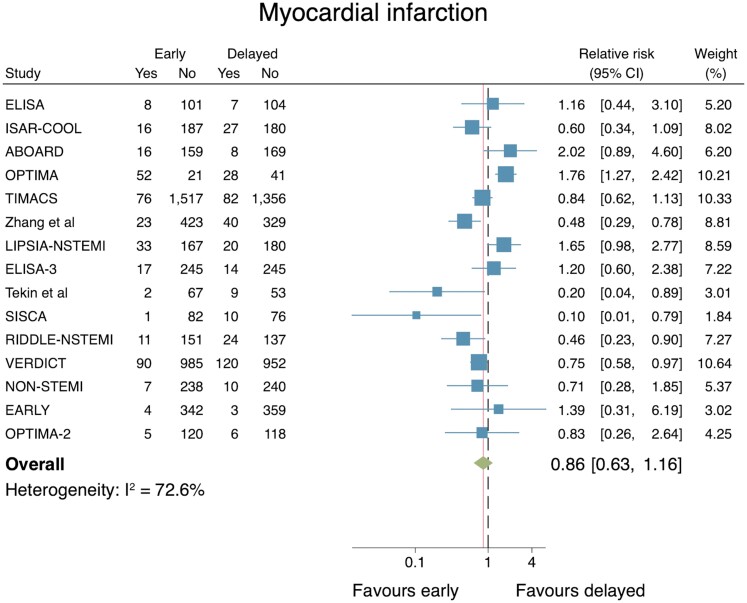
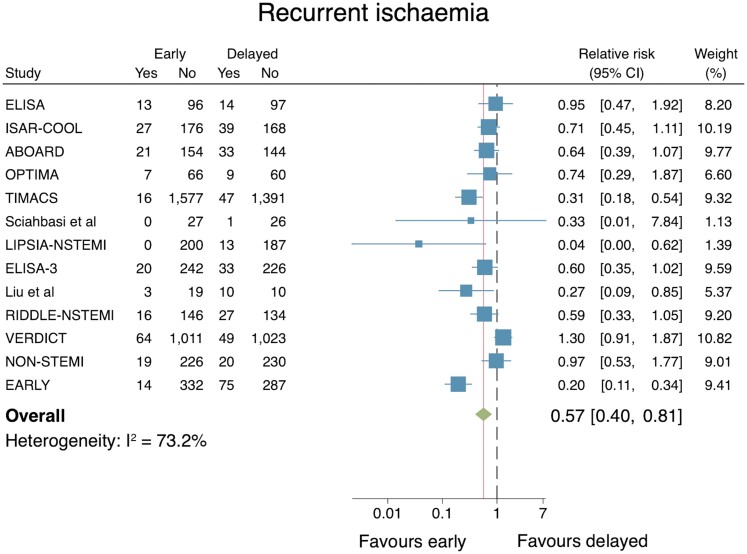
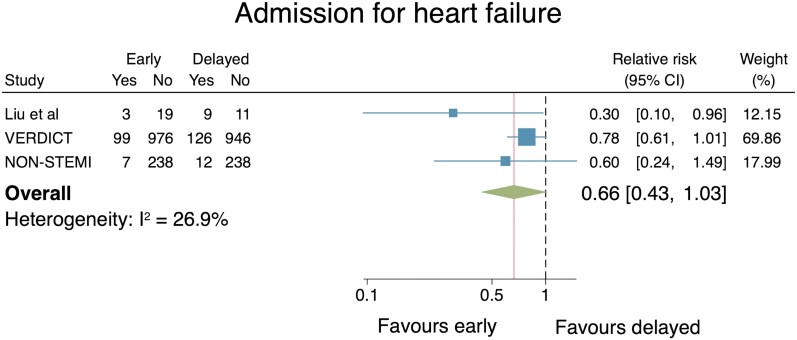
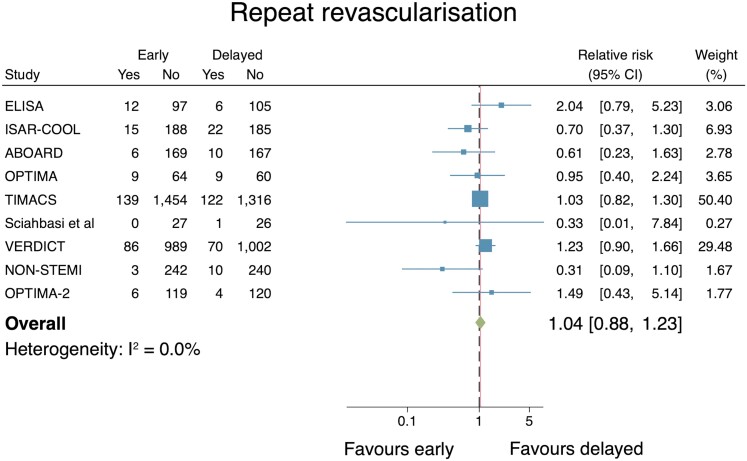
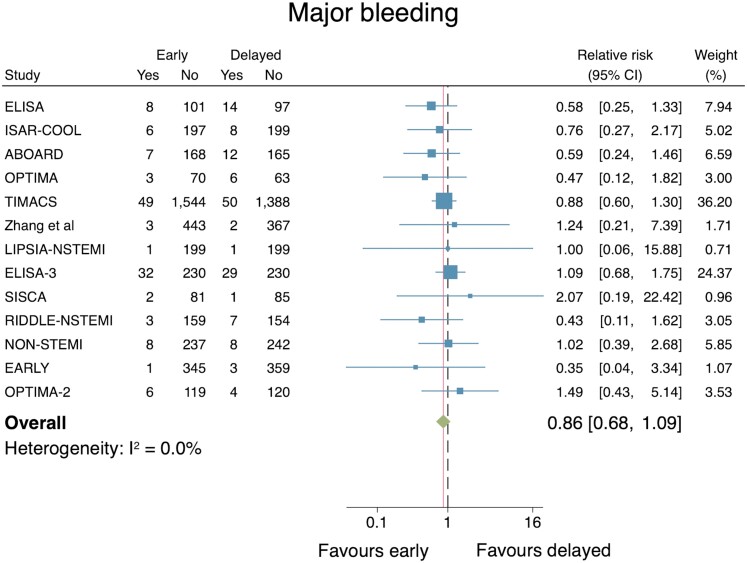
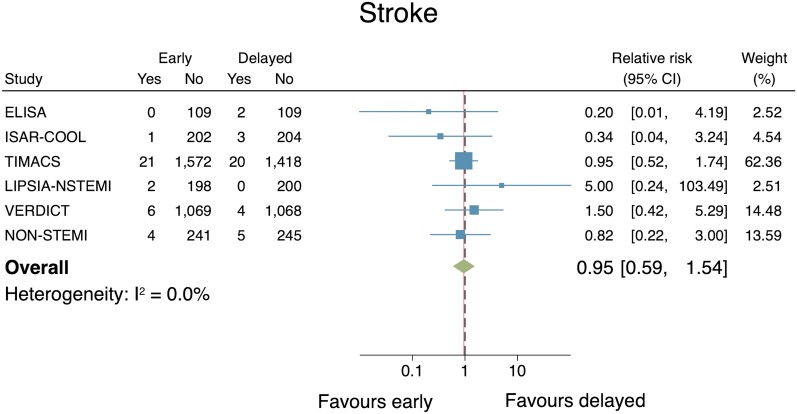
Methods and results: A systematic review of RCTs that compared an early IS vs. delayed IS for NSTE-ACS was conducted by searching MEDLINE, Embase, and Cochrane Central Register of Controlled Trials. A meta-analysis was performed by pooling relative risks (RRs) using a random-effects model. The primary outcome was all-cause mortality. Secondary outcomes included myocardial infarction (MI), recurrent ischaemia, admission for heart failure (HF), repeat re-vascularization, major bleeding, stroke, and length of hospital stay. This study was registered with PROSPERO (CRD42021246131). Seventeen RCTs with outcome data from 10 209 patients were included. No significant differences in risk for all-cause mortality [RR: 0.90, 95% confidence interval (CI): 0.78-1.04], MI (RR: 0.86, 95% CI: 0.63-1.16), admission for HF (RR: 0.66, 95% CI: 0.43-1.03), repeat re-vascularization (RR: 1.04, 95% CI: 0.88-1.23), major bleeding (RR: 0.86, 95% CI: 0.68-1.09), or stroke (RR: 0.95, 95% CI: 0.59-1.54) were observed. Recurrent ischaemia (RR: 0.57, 95% CI: 0.40-0.81) and length of stay (median difference: -22 h, 95% CI: -36.7 to -7.5 h) were reduced with an early IS.
Conclusion: In all-comers with NSTE-ACS, an early IS does not reduce all-cause mortality, MI, admission for HF, repeat re-vascularization, or increase major bleeding or stroke when compared with a delayed IS. Risk of recurrent ischaemia and length of stay are significantly reduced with an early IS.
Keywords: Invasive; Mortality; Non-ST-elevation acute coronary syndrome; Percutaneous coronary intervention; Timing.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: S.A.K. reports personal fees from Bayer. C.P.G. reports personal fees from AstraZeneca, personal fees from Amgen, personal fees from Bayer, grants from BMS, personal fees from Boehrinher-Ingelheim, personal fees from Chiesi, personal fees from Daiichi Sankyo, personal fees from Vifor Pharma, grants from Abbott, personal fees from Menarini, personal fees from Wondr Medical, personal fees from Raisio Group, personal fees from Zydus, personal fees from Oxford University Press, grants from Abbott Diabetes, grants from BMS grants from British Heart Foundation, grants from NIHR, grant from Horizon 2020, grants from ESC, outside the submitted work. N.C. reports unrestricted research grants from Boston Scientific, HeartFlow, Beckman Coulter, and speaker/consultancy fees from Boston, Abbott, HeartFlow outside the submitted work. A.P.B. reports speaker fees from Boston Scientific, Medtronic, Abbott, and Miracor. G.P.M. reports research grants from NIHR, BHF, MRC, and AstraZeneca outside the submitted the work. The remaining authors have no conflicts of interest to declare.
Figures
Comment in
-
Timing of invasive management of NSTE-ACS: is the time up for early management?Eur Heart J. 2022 Sep 1;43(33):3161-3163. doi: 10.1093/eurheartj/ehac212. Eur Heart J. 2022. PMID: 35513989 No abstract available.
-
Timing of early invasive strategy in patients with non-ST-elevation acute coronary syndrome.Eur Heart J. 2022 Nov 21;43(44):4660. doi: 10.1093/eurheartj/ehac466. Eur Heart J. 2022. PMID: 36056878 No abstract available.
-
Timing of invasive strategy in non-ST-elevation acute coronary syndrome: risk and reward?Eur Heart J. 2022 Nov 21;43(44):4661. doi: 10.1093/eurheartj/ehac467. Eur Heart J. 2022. PMID: 36056880 No abstract available.
References
-
- Collet JP, Thiele H, Barbato E, Bauersachs J, Dendale P, Edvardsen T, et al. . 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J 2021;42:1289–1367. - PubMed
-
- Amsterdam EA, Wenger NK, Brindis RG, Casey DE, Ganiats TG, Holmes DR, et al. . 2014 AHA/ACC Guideline for the Management of Patients With Non–ST-Elevation Acute Coronary Syndromes: Executive Summary. Circulation 2014;130:2354–2394. - PubMed
-
- Mehta S, Cannon CP, Fox KAA, Wallentin L, Boden WE, Spacek R, et al. . Routine vs selective invasive strategies in patients with acute coronary syndromes: a collaborative meta-analysis of randomized trials. JAMA 2005;293:2908–2917. - PubMed
-
- Monroe VS, Kerensky RA, Rivera E, Smith KM, Pepine CJ. Pharmacologic plaque passivation for the reduction of recurrent cardiac events in acute coronary syndromes. J Am Coll Cardiol 2003;41:S23–S30. - PubMed
-
- Bonello L, Laine M, Puymirat E, Lemesle G, Thuny F, Paganelli F, et al. . Timing of coronary invasive strategy in non-ST-segment elevation acute coronary syndromes and clinical outcomes: an updated meta-analysis. JACC Cardiovasc Interv 2016;9:2267–2276. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
