

Cadaveric study to assess the feasibility of S1 neurectomy and contralateral S1 transfer for spastic hemiparesis
- PMID: 35514531
- PMCID: PMC9061612
- DOI: 10.1016/j.jor.2022.04.010
Cadaveric study to assess the feasibility of S1 neurectomy and contralateral S1 transfer for spastic hemiparesis
Abstract
Purpose: Acquired brain injury causing spasticity, pain and loss of function is a major cause of disability and lower quality of life. Sacral 1 (S1) neurectomy claims promising outcomes in spastic hemiparesis. This cadaveric study was conducted to study the surgical anatomy, surgical approach and feasibility of S1 neurectomy and contralateral S1 (cS1) transfer.
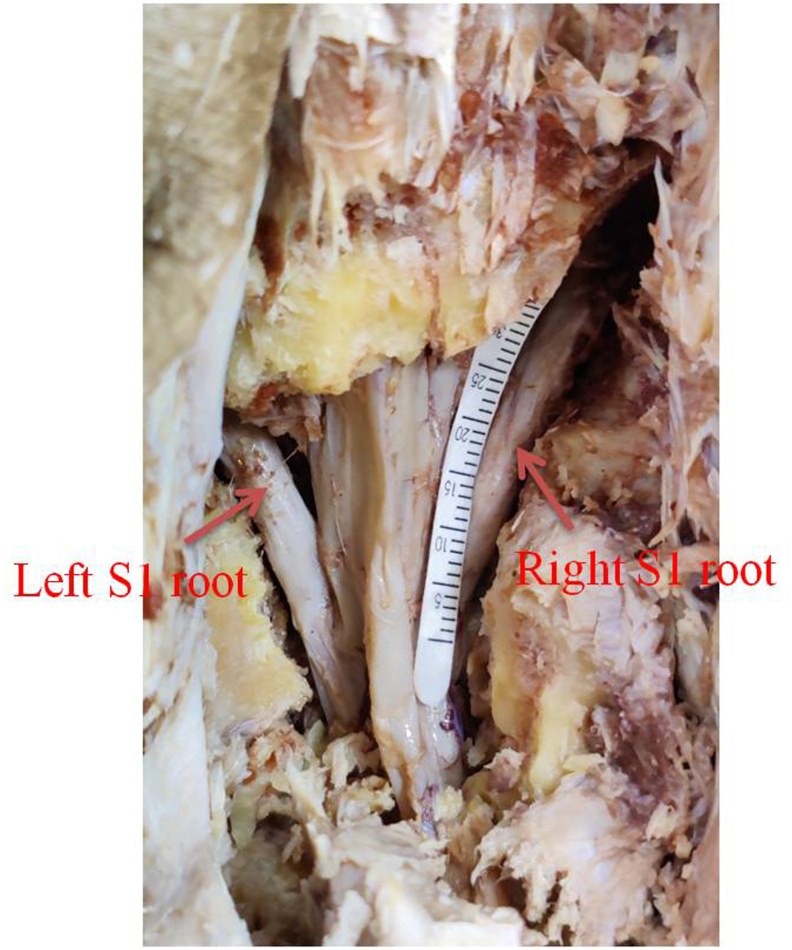
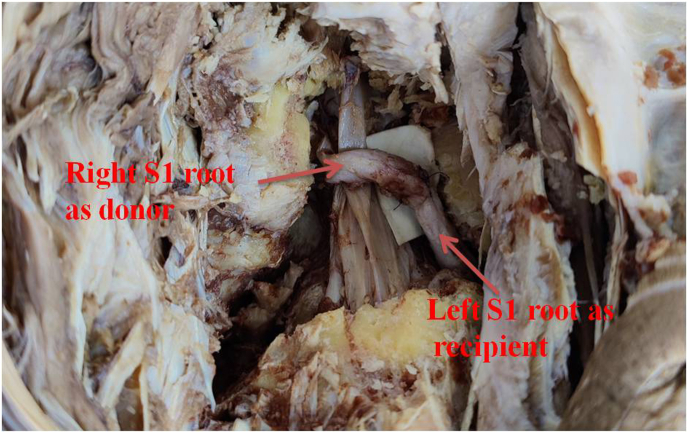
Methods: This study was conducted over a period of 10 months and 10 cadavers (age 18-60 years, 7 male and 3 female) were included in the study. 2 cadavers underwent endoscopic S1 neurectomy and 8 cadavers underwent open S1 neurectomy. Mean S1 root length and diameter were recorded using Schirmer tear strips and Vernier calliper. Feasibility of transfer was also assessed by measuring the length of donor nerve and distance between distal ends to proximal end of recipient nerve.
Results: Mean thickness of right S1 root was 4.02 ± 1.5 mm and left S1 was 3.89 ± 1.18 mm. Mean length of right S1 root was 24.9 ± 4.56 mm and left S1 was 23.6 ± 2.86 mm. Endoscopically dissected length of S1 was much less as compared to open technique.
Conclusion: S1 neurectomy is simple procedure to reduce spasticity in lower limb without any permanent deficit. It can be done by open as well as with endoscopic approach while for contralateral S1 transfer open approach need to be used.
Keywords: Cadaveric; S1 neurectomy; Spastic hemiparesis; cS1transfer.
© 2022 Professor P K Surendran Memorial Education Foundation. Published by Elsevier B.V. All rights reserved.
Figures
Similar articles
-
Extradural contralateral S1 nerve root transfer for spastic lower limb paralysis.J Biomed Res. 2023 Sep 28;37(5):394-400. doi: 10.7555/JBR.37.20230068. J Biomed Res. 2023. PMID: 37750309 Free PMC article.
-
Nerve transfer in the spastic upper limb: anatomical feasibility study.Surg Radiol Anat. 2022 Feb;44(2):183-190. doi: 10.1007/s00276-021-02810-w. Epub 2021 Aug 18. Surg Radiol Anat. 2022. PMID: 34406434
-
Extradural Contralateral C7 Nerve Root Transfer in a Cervical Posterior Approach for Treating Spastic Limb Paralysis: A Cadaver Feasibility Study.Spine (Phila Pa 1976). 2020 Jun 1;45(11):E608-E615. doi: 10.1097/BRS.0000000000003349. Spine (Phila Pa 1976). 2020. PMID: 31770316
-
Selective Neurectomy for the Spastic Upper Extremity.Hand Clin. 2018 Nov;34(4):537-545. doi: 10.1016/j.hcl.2018.06.010. Hand Clin. 2018. PMID: 30286968 Review.
-
Minimally invasive far lateral microendoscopic discectomy for extraforaminal disc herniation at the lumbosacral junction: cadaveric dissection and technical case report.Spine J. 2007 Jul-Aug;7(4):414-21. doi: 10.1016/j.spinee.2006.07.008. Epub 2007 Jan 30. Spine J. 2007. PMID: 17630139 Review.
Cited by
-
Peripheral nerve transfers for dysfunctions in central nervous system injuries: a systematic review.Int J Surg. 2024 Jun 1;110(6):3814-3826. doi: 10.1097/JS9.0000000000001267. Int J Surg. 2024. PMID: 38935818 Free PMC article.
-
Future research focus and trends in nerve transplantation: a bibliometrics research from 2015 to 2024.Front Neurol. 2025 May 22;16:1581859. doi: 10.3389/fneur.2025.1581859. eCollection 2025. Front Neurol. 2025. PMID: 40474921 Free PMC article.
-
Application of CT images for reconstruction of adigital model of the sacral nerve canal.Am J Transl Res. 2024 Nov 15;16(11):7087-7095. doi: 10.62347/SRDD6372. eCollection 2024. Am J Transl Res. 2024. PMID: 39678589 Free PMC article.
References
-
- Mou Xianong, Zheng, et al. Trial of contralateral seventh cranial nerve transfer for spastic arm paralysis. N Engl J Med. 2017;20:72–74. - PubMed
-
- Zhu L., Zhang F., Yang D., Chen A. The effect of severing a normal s1 nerve root to use for reconstruction of an avulsed contralateral lumbosacral plexus. The bone joint J. 2014:358–365. - PubMed
-
- Bishop B. Spasticity: its physiology and management. Part II. Neurophysiology of spasticity: current concepts. Phys Ther. 1977;57:377–384. - PubMed
-
- Kischka U. Neurological rehabilitation and management of spasticity. Medicine. 2008;36:616–619.
LinkOut - more resources
Full Text Sources
Miscellaneous
